

Case Reports
doi: 10.1016/j.case.2022.10.004.
eCollection 2023 Jan.
Left Atrial Appendage Occlusion Device Buckling: An Avoidable Deployment Complication Identified and Corrected Using Intraprocedural Transesophageal Echocardiography
Affiliations
- PMID: 36704483
- PMCID: PMC9871351
- DOI: 10.1016/j.case.2022.10.004
Item in Clipboard
Case Reports
Left Atrial Appendage Occlusion Device Buckling: An Avoidable Deployment Complication Identified and Corrected Using Intraprocedural Transesophageal Echocardiography
CASE (Phila).
.
No abstract available
Keywords: Deployment complication; Left atrial appendage occlusion; Procedural transesophageal echocardiography; Watchman device.
Figures
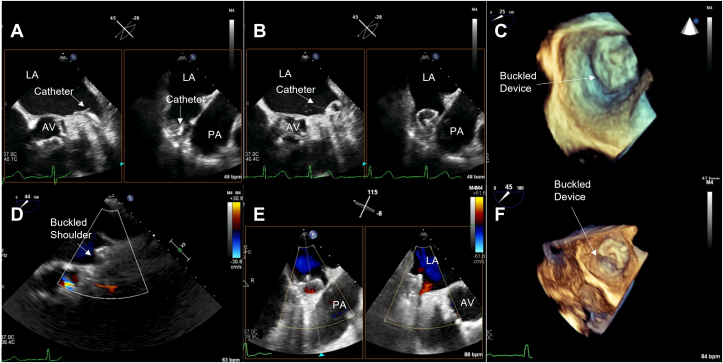
Midesophageal TEE Images from case 1: (A) 2D x-plane view at 45° showing the acute angle of deployment catheter positioned into the LAA; (B) 2D x-plane view at 45° showing LAAO device buckle immediately after deployment; (C) 3D view at 25° showing collapse of device shoulder immediately after deployment; (D) 2D view with color Doppler at 44° showing the buckle at 45 days postimplantation; (E) 2D x-plane view at 115° showing device buckling and color Doppler evidence of peridevice leak at 1-year postimplantation; (F) 3D view at 45° showing device the buckle at 1-year postimplantation. AV, aortic valve; LA, left atrium; PA, pulmonary artery.
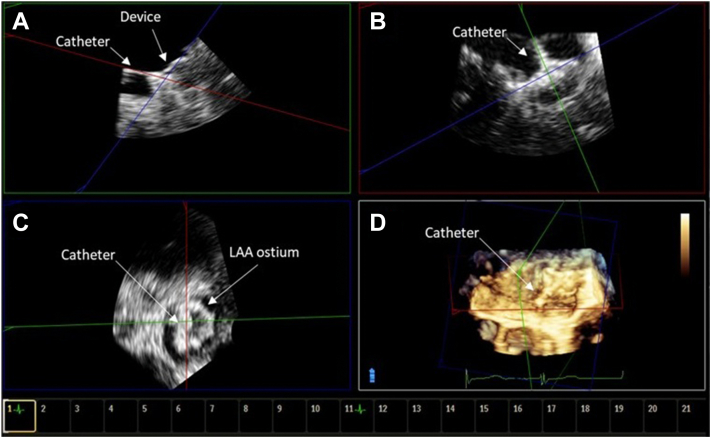
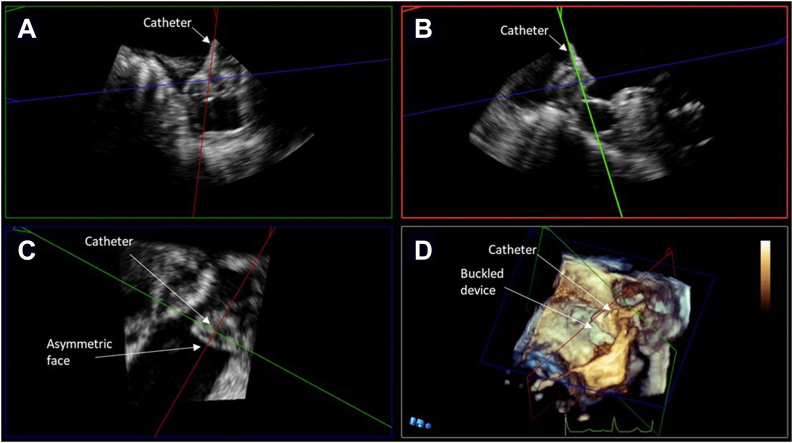
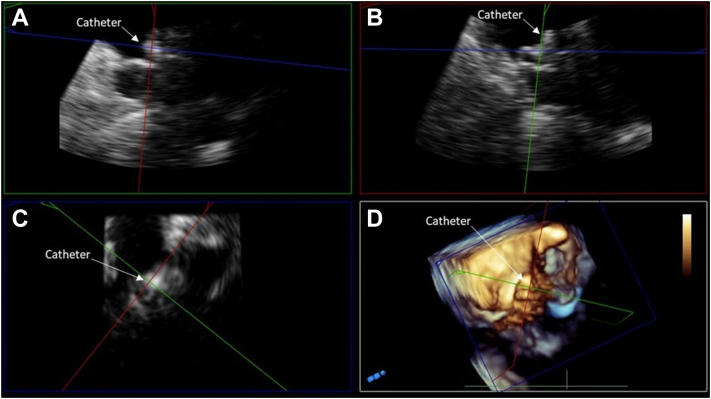
TEE MPR image from case 1. (A) Orthogonal postacquisition MPR images showing noncoaxial orientation of the catheter relative to the axis of the LAA. (B) The deployment catheter is coaxial to the LAA ostium. (C) Lack of coaxial orientation, which is noted in panel A, led to an asymmetric shape of the device face. (D) Three-dimensional view showing noncoaxial deployment catheter orientation.
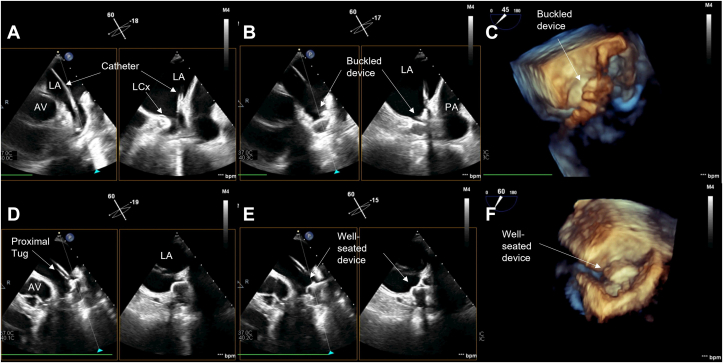
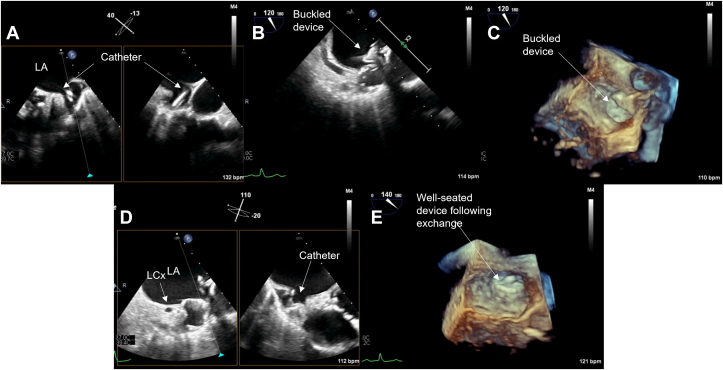
Midesophageal TEE images from case 2: (A) 2D x-plane view at 60° showing acute angle of deployment catheter into LAA; (B) 2D x-plane view at 60° showing LAAO device buckling immediately after deployment; (C) 3D view at 45° showing buckling immediately after deployment; (D) 2D x-plane view at 60° showing proximal tug to relieve collapsed portion of the device face; (E) 2D x-plane view at 60° showing relieved buckle; (F) 3D view at 60° showing well-seated device. AV, aortic valve; LA, left atrium; LCx, left circumflex coronary artery; PA, pulmonary artery.
TEE MPR image from case 2. (A) Postacquisition MPR images showing noncoaxial orientation of the deployment catheter to the LAA ostium. (B) Note that the deployment catheter appears more coaxial following a proximal tug. (C) Asymmetric device face noted due to buckle on initial deployment before proximal tug. (D) Three-dimensional image showing buckled device face before proximal tug maneuver.
Midesophageal TEE images from case 3: (A) 2D x-plane view at 40° showing acute angle of deployment catheter into LAA; (B) 2D view at 120° showing LAAO device buckle immediately after deployment; (C) 3D view at 120° showing buckling immediately after deployment; (D) 2D x-plane view at 110° showing less acute deployment catheter angle and well-seated device after initial device recapture; (E) 3D view at 140° showing well-seated device. LA, Left atrium; LCx, left circumflex coronary artery.
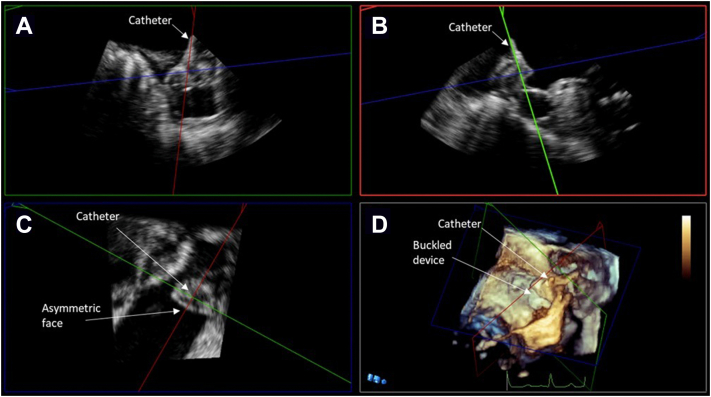
TEE MPR image from case 3. (A) Postacquisition MPR images showing noncoaxial orientation of the deployment catheter to the LAA ostium. (B) Noncoaxial orientation associated with buckled device. (C) Asymmetric device face before smaller device was exchanged. (D) Three-dimensional image of buckling with defect toward the mitral shoulder of the device.
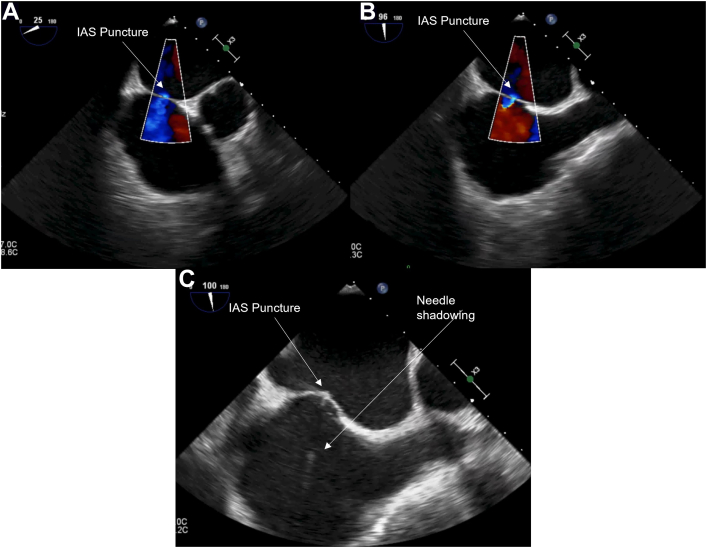
Midesophageal images of transseptal puncture: (A) 2D view at 25° showing the transeptal puncture and associated color Doppler; (B) 2D view at 96° showing the transeptal puncture and associated color Doppler; (C) 2D view at 100° showing the transeptal puncture with needle shadowing present. IAS, interatrial septum.
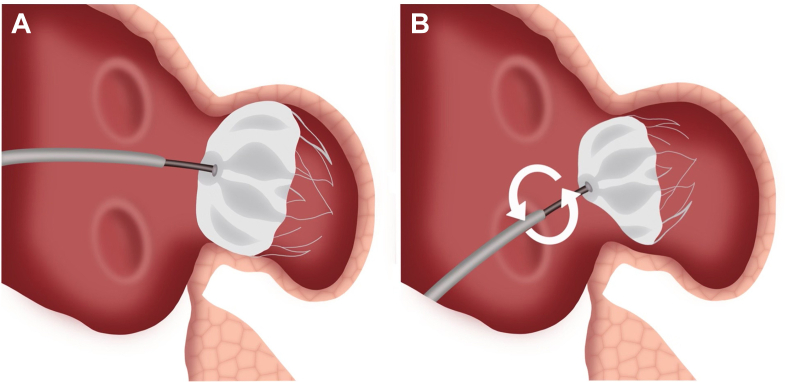
Buckling graphic. (A) Correct demonstration of LAAO device insertion. Deployment catheter and device face are coaxial to the axis of the LAA and the LAA ostium. The device is well seated. (B) Suboptimal transeptal puncture leads to acute angle between deployment catheter and device face within the LAA. Under torque applied to improve device seating, the device can buckle, resulting in collapse shoulder and an apparent buckle in the face of the device. This could lead to a peridevice leak.
Similar articles
-
Evaluating the role of transesophageal echocardiography (TEE) or intracardiac echocardiography (ICE) in left atrial appendage occlusion: a meta-analysis.J Interv Card Electrophysiol. 2021 Jan;60(1):41-48. doi: 10.1007/s10840-019-00677-x. Epub 2020 Jan 17. J Interv Card Electrophysiol. 2021. PMID: 31953708
-
Left atrial appendage closure with the Watchman device using intracardiac vs transesophageal echocardiography: Procedural and cost considerations.Heart Rhythm. 2019 Mar;16(3):334-342. doi: 10.1016/j.hrthm.2018.12.013. Heart Rhythm. 2019. PMID: 30827462 Free PMC article.
-
Intraprocedural and long-term incomplete occlusion of the left atrial appendage following placement of the WATCHMAN device: a single center experience.J Cardiovasc Electrophysiol. 2012 May;23(5):455-61. doi: 10.1111/j.1540-8167.2011.02216.x. Epub 2011 Nov 14. J Cardiovasc Electrophysiol. 2012. PMID: 22082312
-
Left Atrial Appendage Occlusion/Exclusion: Procedural Image Guidance with Transesophageal Echocardiography.J Am Soc Echocardiogr. 2018 Apr;31(4):454-474. doi: 10.1016/j.echo.2017.09.014. Epub 2017 Nov 20. J Am Soc Echocardiogr. 2018. PMID: 29158017 Review.
-
Accuracy of Commonly-Used Imaging Modalities in Assessing Left Atrial Appendage for Interventional Closure: Review Article.J Clin Med. 2018 Nov 14;7(11):441. doi: 10.3390/jcm7110441. J Clin Med. 2018. PMID: 30441824 Free PMC article. Review.
Cited by
-
Three-dimensional multiplanar reconstruction by transoesophageal echocardiography showed inside reverse fold: "origami" shape of WATCHMAN FLX.AsiaIntervention. 2024 Feb 29;10(1):64-65. doi: 10.4244/AIJ-D-23-00032. eCollection 2024 Feb. AsiaIntervention. 2024. PMID: 38425809 Free PMC article. No abstract available.
References
-
- Reddy V., Doshi S., Kar S., Gibson D., Price M., Huber k., et al. 5-year outcomes after left atrial appendage closure. J Am Coll Cardiol. 2017;70:2964–2975. - PubMed
-
- Chue C.D., de Giovanni J., Steeds R.P. The role of echocardiography in percutaneous left atrial appendage occlusion. Eur J Echocardiogr. 2011;12:i3–i10. - PubMed
-
- Holmes D.R., Reddy V., Turi Z., Doshi S., Sievert H., Buchbinder M., et al. Percutaneous closure of the left atrial appendage versus warfarin therapy for prevention of stroke in patients with atrial fibrillation: a randomised non-inferiority trial. Lancet. 2009;374:534–542. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
