

Case Reports
doi: 10.1016/j.case.2022.09.008.
eCollection 2023 Jan.
Transcatheter Edge-to-Edge Repair for Left Atrioventricular Valve Cleft After Previously Repaired Complete Atrioventricular Canal Defect in Down Syndrome
Affiliations
- PMID: 36704485
- PMCID: PMC9871344
- DOI: 10.1016/j.case.2022.09.008
Item in Clipboard
Case Reports
Transcatheter Edge-to-Edge Repair for Left Atrioventricular Valve Cleft After Previously Repaired Complete Atrioventricular Canal Defect in Down Syndrome
CASE (Phila).
.
No abstract available
Keywords: Cleft leaflet; Down syndrome; Mitral regurgitation; Percutaneous mitral valve repair; Transcatheter edge-to-edge repair.
Figures
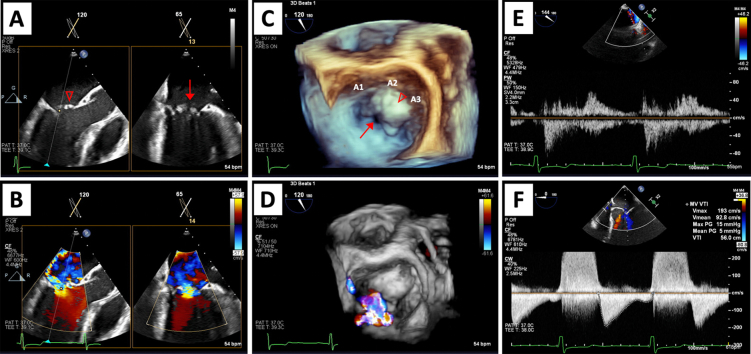
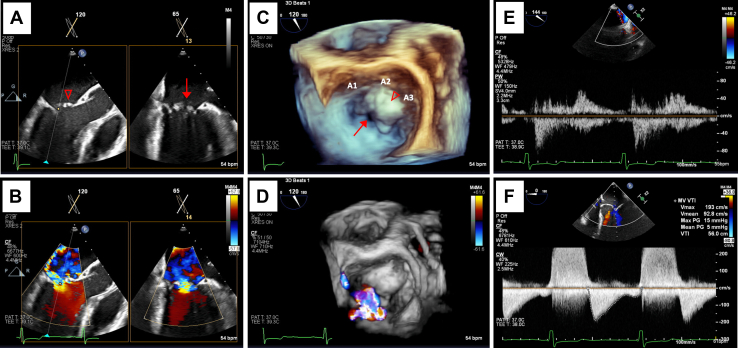
Baseline intraprocedural TEE images. Midesophageal biplane imaging of a long-axis and bicommissural view without and with color Doppler (A, B), three-dimensional surgeon's view without and with color Doppler demonstrating severe regurgitation (C, D), systolic flow reversal in the right upper pulmonary vein (E), and elevated transvalvular inflow gradients (F). Anterior leaflet cleft (↓) and A2/A3 prolapse (∇) are shown in 2D (A) and three-dimensional (C) imaging.
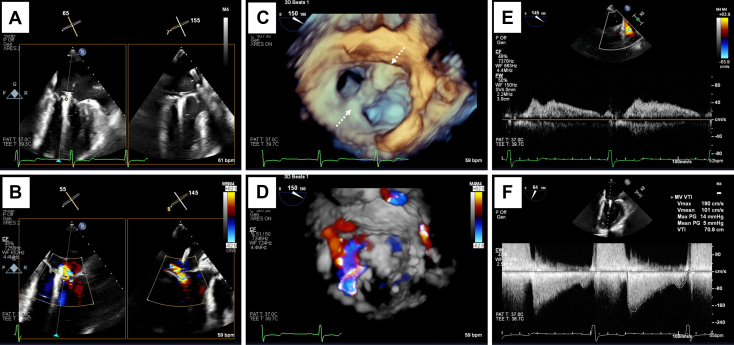
Post-TEER intraprocedural TEE images. Midesophageal biplane imaging of a long-axis and bicommissural view without and with color Doppler demonstrating bileaflet capture with reduction to mild-moderate regurgitation (A, B), three-dimensional surgeon's view demonstrating angulated device positioning (dashed arrows) with tissue bridge and color Doppler (C, D), right upper pulmonary vein subsequently with systolic dominant flow (E), and stable transvalvular inflow gradients following device release (F).
Similar articles
-
Surgically created double-orifice left atrioventricular valve: a valve-sparing repair in selected atrioventricular septal defects.J Thorac Cardiovasc Surg. 2001 Feb;121(2):352-64. doi: 10.1067/mtc.2001.111969. J Thorac Cardiovasc Surg. 2001. PMID: 11174742
-
Percutaneous edge-to-edge repair for common atrioventricular valve regurgitation in a patient with heterotaxy syndrome, single ventricle physiology, and unbalanced atrioventricular septal defect.Catheter Cardiovasc Interv. 2020 Aug;96(2):384-388. doi: 10.1002/ccd.28782. Epub 2020 Feb 19. Catheter Cardiovasc Interv. 2020. PMID: 32073720
-
Cleft of the mitral valve in patients with Down's syndrome.Cardiol Young. 2002 Jan;12(1):27-31. doi: 10.1017/s1047951102000057. Cardiol Young. 2002. PMID: 11922437
-
Percutaneous approaches to valve repair for mitral regurgitation.J Am Coll Cardiol. 2014 May 27;63(20):2057-2068. doi: 10.1016/j.jacc.2014.01.039. Epub 2014 Feb 26. J Am Coll Cardiol. 2014. PMID: 24583296 Review.
-
Recent advances in patient selection and devices for transcatheter edge-to-edge mitral valve repair in heart failure.Expert Rev Med Devices. 2020 Feb;17(2):93-102. doi: 10.1080/17434440.2020.1714433. Epub 2020 Jan 21. Expert Rev Med Devices. 2020. PMID: 31923376 Review.
Cited by
-
Introduction of transcatheter edge-to-edge repair in patients with congenital heart disease at a children's hospital.Catheter Cardiovasc Interv. 2024 Feb;103(2):326-334. doi: 10.1002/ccd.30935. Epub 2023 Dec 27. Catheter Cardiovasc Interv. 2024. PMID: 38149722 Free PMC article.
References
-
- Otto C.M., Nishimura R.A., Bonow R.O., Carabello B.A., Erwin J.P., 3rd, Gentile F., et al. 2020 ACC/AHA guideline for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2021;143:e72–e227. - PubMed
-
- Artrip J.H., Rumball E.M., Finucane K. Repair of left atrioventricular valve cleft defects with patch augmentation. Ann Thorac Surg. 2012;93:2081–2083. - PubMed
-
- Van Praagh S., Porras D., Oppido G., Geva T., Van Praagh R. Cleft mitral valve without ostium primum defect: anatomic data and surgical considerations based on 41 cases. Ann Thorac Surg. 2003;75:1752–1762. - PubMed
