

Societal costs associated with pulmonary arterial hypertension: A study utilizing linked national registries
- PMID: 36704610
- PMCID: PMC9868346
- DOI: 10.1002/pul2.12190
Societal costs associated with pulmonary arterial hypertension: A study utilizing linked national registries
Abstract
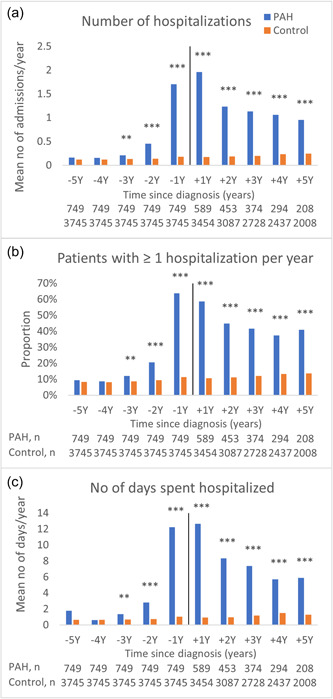
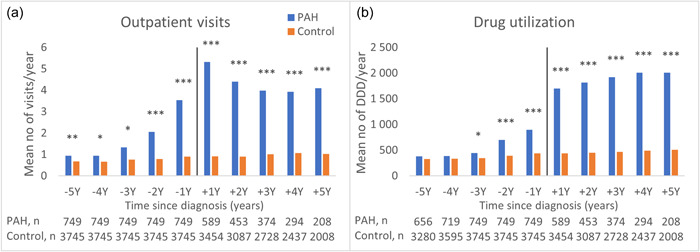
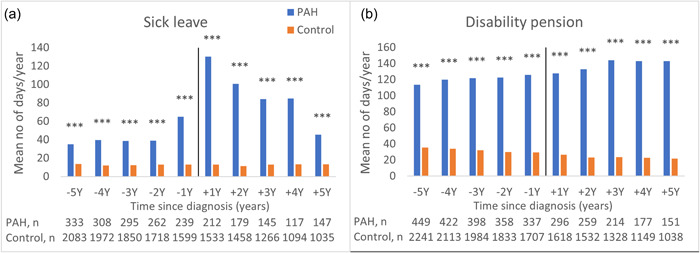
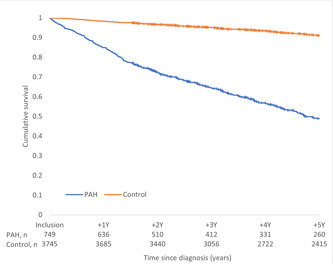
Pulmonary arterial hypertension (PAH) is a progressive disease with no cure. Healthcare resource utilization (HCRU; hospitalization, outpatient visits, and drug utilization) before diagnosis and productivity loss (sick leave and disability pension) before and after PAH diagnosis are not well known. By linking several Swedish national databases, this study have estimated the societal costs in a national PAH cohort (n = 749, diagnosed with PAH in 2008-2019) 5 years before and 5 years after diagnosis and compared to an age, sex, and geographically matched control group (n = 3745, 1:5 match). HCRU and productivity loss were estimated per patient per year. The PAH group had significantly higher HCRU and productivity loss compared to the control group starting already 3 and 5 years before diagnosis, respectively. HCRU peaked the year after diagnosis in the PAH group with hospitalizations (mean ± standard deviation; 2.0 ± 0.1 vs. 0.2 ± 0.0), outpatient visits (5.3 ± 0.3 vs. 0.9 ± 0.1), and days on sick leave (130 ± 10 vs. 13 ± 1) significantly higher compared to controls. Total costs during the entire 10-year period were six times higher for the PAH group than the control group. In the 5 years before diagnosis the higher costs were driven by productivity loss (76%) and hospitalizations (15%), while the 5 years after diagnosis the main cost drivers were drugs (63%), hospitalizations (16%), and productivity loss (16%). In conclusion, PAH was associated with large societal costs due to high HCRU and productivity loss, starting several years before diagnosis. The economic and clinical burden of PAH suggests that strategies for earlier diagnosis and more effective treatments are warranted.
Keywords: healthcare resource utilization; national registry; productivity loss; pulmonary hypertension.
© 2023 The Authors. Pulmonary Circulation published by John Wiley & Sons Ltd on behalf of Pulmonary Vascular Research Institute.
Conflict of interest statement
Amélie Beaudet and Nadia Pillai are employees of Actelion Pharmaceuticals, a Janssen Pharmaceutical Company of Johnson & Johnson, Allschwil, Switzerland. The remaining authors declare no conflict of interest.
Figures
Similar articles
-
Societal costs associated to chronic thromboembolic pulmonary hypertension: A study utilizing linked national registries.Pulm Circ. 2023 Jun 22;13(2):e12254. doi: 10.1002/pul2.12254. eCollection 2023 Apr. Pulm Circ. 2023. PMID: 37362560 Free PMC article.
-
Societal Costs Associated With Pulmonary Arterial Hypertension Subgroups: A Study Utilizing Linked National Registries.Pulm Circ. 2025 Apr 17;15(2):e70074. doi: 10.1002/pul2.70074. eCollection 2025 Apr. Pulm Circ. 2025. PMID: 40248212 Free PMC article.
-
Excess healthcare resource utilization and costs for commercially insured patients with pulmonary arterial hypertension: A real-world data analysis.Pulm Circ. 2024 Jun 19;14(2):e12390. doi: 10.1002/pul2.12390. eCollection 2024 Apr. Pulm Circ. 2024. PMID: 38903484 Free PMC article.
-
Economic burden of pulmonary arterial hypertension (PAH) and chronic thromboembolic pulmonary hypertension (CTEPH) in Finland.Int J Cardiol Heart Vasc. 2024 Oct 22;55:101534. doi: 10.1016/j.ijcha.2024.101534. eCollection 2024 Dec. Int J Cardiol Heart Vasc. 2024. PMID: 39507296 Free PMC article.
-
Burden of pulmonary arterial hypertension in England: retrospective HES database analysis.Ther Adv Respir Dis. 2021 Jan-Dec;15:1753466621995040. doi: 10.1177/1753466621995040. Ther Adv Respir Dis. 2021. PMID: 33620026 Free PMC article.
Cited by
-
Circulating biomarkers in pulmonary arterial hypertension: State-of-the-art review and future directions.JHLT Open. 2024 Aug 23;6:100152. doi: 10.1016/j.jhlto.2024.100152. eCollection 2024 Nov. JHLT Open. 2024. PMID: 40145036 Free PMC article. Review.
-
Pulmonary Hypertension: Pharmacological and Non-Pharmacological Therapies.Life (Basel). 2024 Oct 4;14(10):1265. doi: 10.3390/life14101265. Life (Basel). 2024. PMID: 39459565 Free PMC article. Review.
-
Validation of the Pulmonary Arterial Hypertension-Symptoms and Impact for Clinical Use (SYMPACT-CP): a qualitative interview study.BMC Pulm Med. 2025 May 6;25(1):217. doi: 10.1186/s12890-025-03681-2. BMC Pulm Med. 2025. PMID: 40329256 Free PMC article.
-
Risk Assessment Models and Event-Free Survival in Pulmonary Arterial Hypertension.Pulm Circ. 2025 Jul 18;15(3):e70132. doi: 10.1002/pul2.70132. eCollection 2025 Jul. Pulm Circ. 2025. PMID: 40687338 Free PMC article.
-
The one-minute sit-to-stand-test performance is associated with health-related quality of life in patients with pulmonary hypertension.PLoS One. 2024 May 29;19(5):e0301483. doi: 10.1371/journal.pone.0301483. eCollection 2024. PLoS One. 2024. PMID: 38809846 Free PMC article.
References
-
- Galiè N, Humbert M, Vachiery J‐L, Gibbs S, Lang I, Torbicki A, Simonneau G, Peacock A, Vonk Noordegraaf A, Beghetti M, Ghofrani A, Gomez Sanchez MA, Hansmann G, Klepetko W, Lancellotti P, Matucci M, McDonagh T, Pierard LA, Trindade PT, Zompatori M, Hoeper M, ESC Scientific Document G. 2015 ESC/ERS guidelines for the diagnosis and treatment of pulmonary hypertension: the joint task force for the diagnosis and treatment of pulmonary hypertension of the European Society of Cardiology (ESC) and the European Respiratory Society (ERS): endorsed by: association for European paediatric and congenital cardiology (AEPC), International Society for Heart and Lung Transplantation (ISHLT). Eur Heart J. 2016;37(1):67–119. - PubMed
-
- National Health Service Digital . National pulmonary hypertension audit, 12th annual report. Accessed May 18, 2022. https://digital.nhs.uk/data-and-information/publications/statistical/nat...
-
- SPAHR (Swedish Pulmonary Arterial Registry) . Årsrapport. 2020. Accessed June 1, 2022. https://www.ucr.uu.se/spahr/arsrapporter/arsrapporter/arsrapport-spahr-2020
-
- Rådegran G, Kjellström B, Ekmehag B, Larsen F, Rundqvist B, Blomquist SB, Gustafsson C, Hesselstrand R, Karlsson M, Kornhall B, Nisell M, Persson L, Ryftenius H, Selin M, Ullman B, Wall K, Wikström G, Willehadson M, Jansson K. Characteristics and survival of adult Swedish PAH and CTEPH patients 2000−2014. Scand Cardiovasc J. 2016;50(4):243–50. - PubMed
