

Predictors of Distant Metastasis and Prognosis in Newly Diagnosed T1 Intrahepatic Cholangiocarcinoma
- PMID: 36704724
- PMCID: PMC9873431
- DOI: 10.1155/2023/6638755
Predictors of Distant Metastasis and Prognosis in Newly Diagnosed T1 Intrahepatic Cholangiocarcinoma
Abstract
Background: According to American Joint Committee on Cancer (AJCC) 8th staging system, T1 intrahepatic cholangiocarcinoma (T1 ICC) is considered a tumor with no vascular invasion. However, T1 ICC usually occurs distant metastasis (DM), and the clinical features of these patients could help clinicians identify the high-risk population.
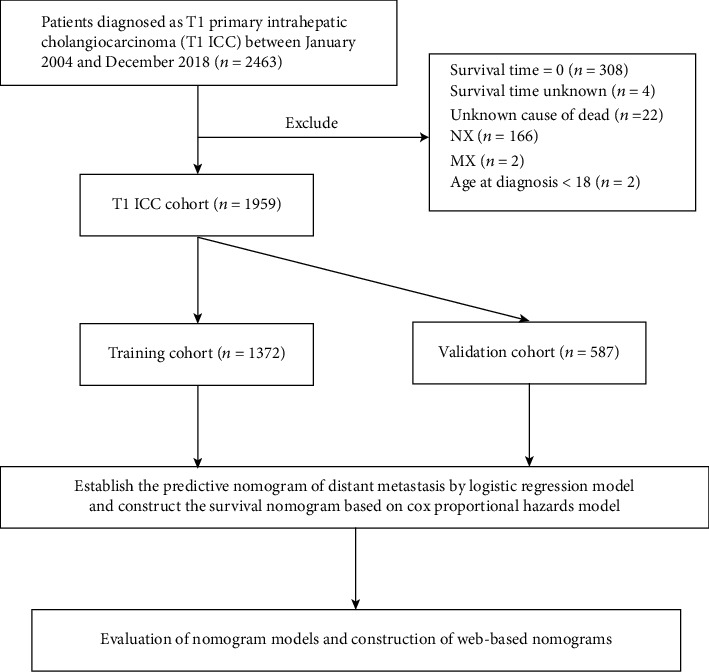
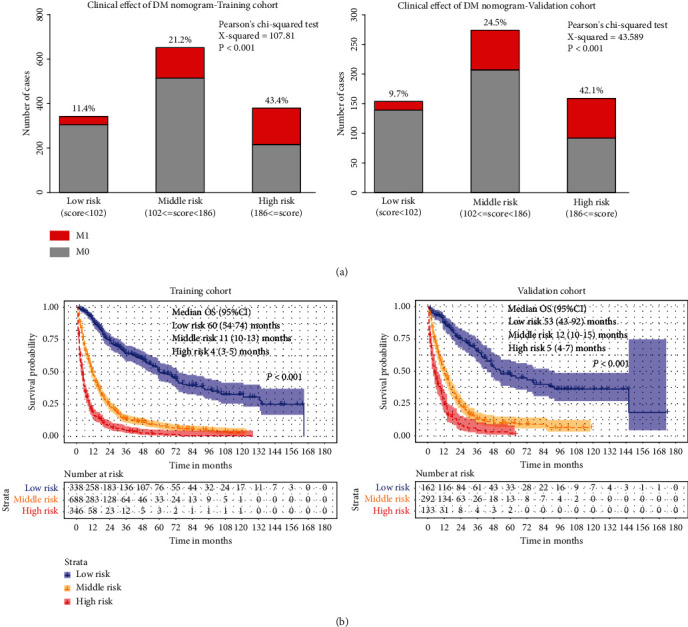
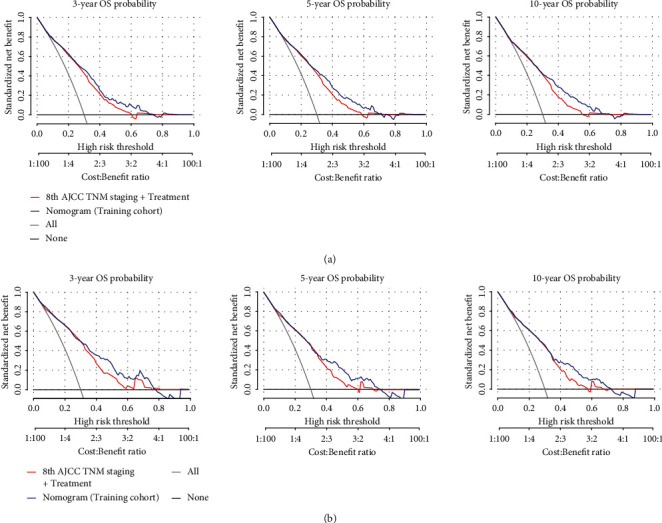
Methods: We reviewed 1959 newly diagnosed patients with T1 ICC from the Surveillance, Epidemiology, and End Results (SEER) database during 2004-2018. Logistic regression models and Cox proportional hazards models were conducted to predict the risk of DM and overall survival (OS), respectively, and then, web-based nomograms were constructed. Decision curve analysis (DCA) and clinical impact curves (CIC) were used to measure the clinical utility of the models. The low-, medium-, and high-risk groups were identified by calculating the summary of the risk points. Nomograms on the web were also created to help clinicians better use these prediction models.
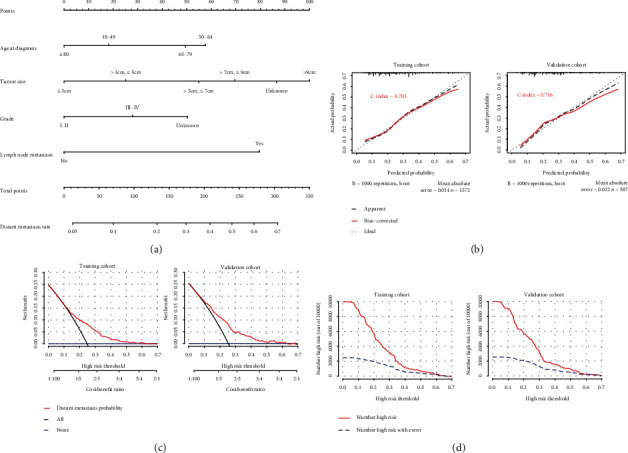
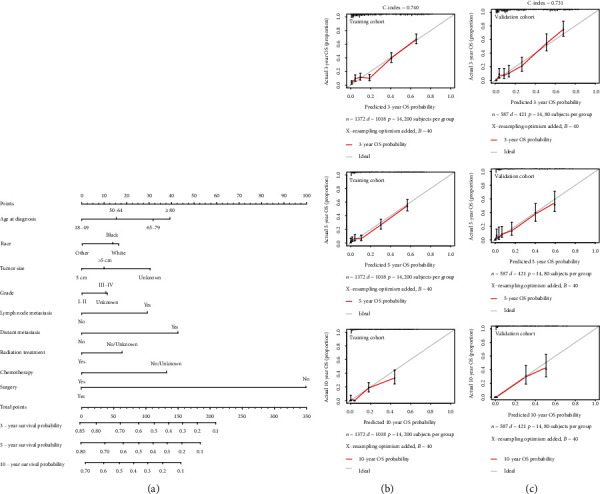
Results: Tumor size and lymph node metastasis accounted for the first two largest proportions among the DM nomogram scores, while surgery, DM, age at diagnosis, chemotherapy, and lymph node metastasis occupied the largest percentage in OS nomogram. DM nomogram was established for these newly diagnosed patients with T1 ICC, and OS nomogram was developed to visually predict the OS rate of 3, 5, and 10 years. The calibration curves revealed a valid predictive accuracy of nomograms, of which the C-index was 0.703 and 0.740, respectively, for good discrimination. DCAs, CICs, and risk subgroups showed the clinical validity of these nomograms. Two websites were created to make it easier to use these nomograms.
Conclusions: Novel web-based nomograms predicting the risk of DM and OS for T1 ICC were constructed. These predictive tools might help clinicians make precise clinical strategies for each patient with T1 ICC.
Copyright © 2023 Kaibo Guo et al.
Conflict of interest statement
The authors state that there is no conflict of interest.
Figures
Similar articles
-
Diagnostic and prognostic nomograms for newly diagnosed intrahepatic cholangiocarcinoma with brain metastasis: A population-based analysis.Exp Biol Med (Maywood). 2022 Sep;247(18):1657-1669. doi: 10.1177/15353702221113828. Epub 2022 Aug 10. Exp Biol Med (Maywood). 2022. PMID: 35946168 Free PMC article.
-
Risk factors and predictors of lymph nodes metastasis and distant metastasis in newly diagnosed T1 colorectal cancer.Cancer Med. 2020 Jul;9(14):5095-5113. doi: 10.1002/cam4.3114. Epub 2020 May 29. Cancer Med. 2020. PMID: 32469151 Free PMC article.
-
A nomogram to predict lymph node metastasis before resection in intrahepatic cholangiocarcinoma.J Surg Res. 2018 Jun;226:56-63. doi: 10.1016/j.jss.2018.01.024. Epub 2018 Feb 10. J Surg Res. 2018. PMID: 29661289
-
Staging of intrahepatic cholangiocarcinoma.Curr Opin Gastroenterol. 2010 May;26(3):269-73. doi: 10.1097/MOG.0b013e328337c899. Curr Opin Gastroenterol. 2010. PMID: 20179593 Review.
-
Staging Systems and Nomograms for Soft Tissue Sarcoma.Curr Oncol. 2023 Mar 26;30(4):3648-3671. doi: 10.3390/curroncol30040278. Curr Oncol. 2023. PMID: 37185391 Free PMC article. Review.
Cited by
-
Prognostic models for mucinous and non-specific adeno cholangiocarcinoma: a population-based retrospective study.Front Endocrinol (Lausanne). 2024 Jun 11;15:1284283. doi: 10.3389/fendo.2024.1284283. eCollection 2024. Front Endocrinol (Lausanne). 2024. PMID: 38919485 Free PMC article.
References
-
- Wu L., Tsilimigras D. I., Paredes A. Z., et al. Trends in the incidence, treatment and outcomes of patients with intrahepatic cholangiocarcinoma in the USA: facility type is associated with margin status, use of lymphadenectomy and overall survival. World Journal of Surgery . 2019;43(7):1777–1787. doi: 10.1007/s00268-019-04966-4. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
