

Ultrasound-guided trans-incisional quadratus lumborum block versus ultrasound-guided caudal analgesia in pediatric open renal surgery: a randomized trial
- PMID: 36704815
- PMCID: PMC10562062
- DOI: 10.4097/kja.22774
Ultrasound-guided trans-incisional quadratus lumborum block versus ultrasound-guided caudal analgesia in pediatric open renal surgery: a randomized trial
Abstract
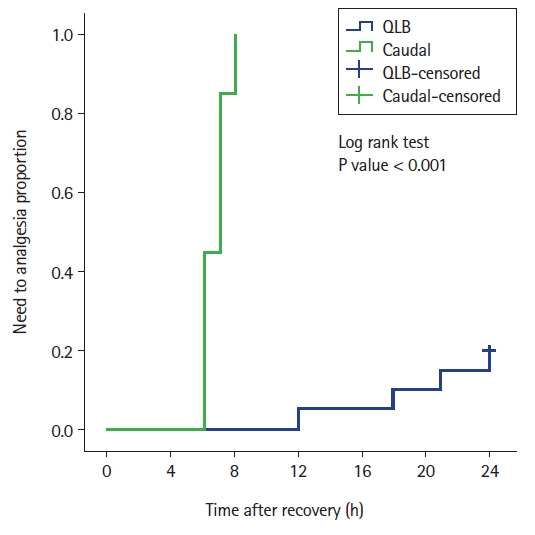
Background: The caudal route is a common approach for postoperative analgesia; however, it is associated with limited duration of action. The quadratus lumborum block (QLB) may produce prolonged postoperative analgesia. Therefore, this study aimed to compare the postoperative analgesic efficacy of the ultrasound-guided caudal block with that of the ultrasound-guided transincisional QLB (TiQLB) in pediatric patients undergoing open renal surgery.
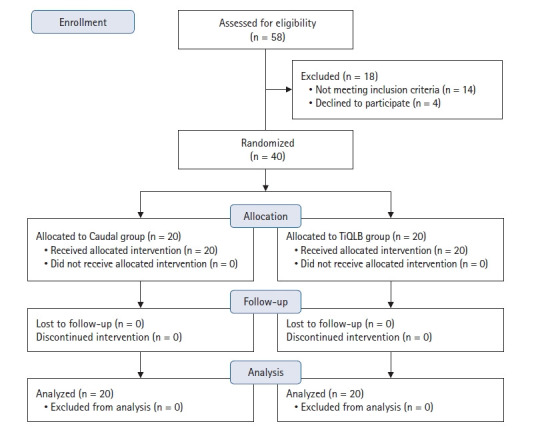
Methods: Forty patients of both sexes, aged 2-11 years, were randomly assigned to receive either caudal analgesia with 1.25 ml/kg of bupivacaine 0.2% (Caudal group; n = 20) or a QLB with 0.5 ml/kg of bupivacaine 0.2% (TiQLB group; n = 20) in addition to standard general anesthesia. Time to first analgesia was the primary outcome. Total analgesic consumption in the first 24 h postoperatively, pain scores, and the incidence of side effects were the secondary outcomes.
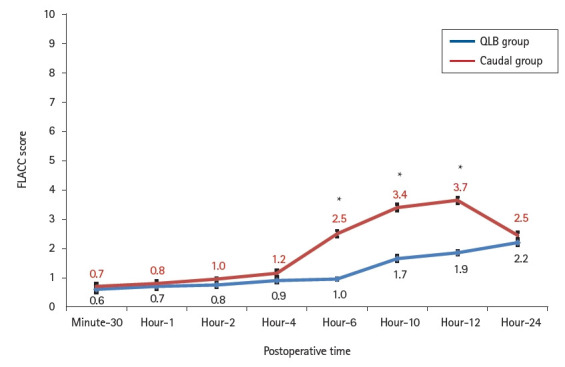
Results: The mean time to first analgesic requirement was significantly longer in the TiQLB group than in the Caudal group (18.8 ± 5.1 vs. 6.7 ± 0.7 h, P < 0.001). Total ketorolac consumption and pain scores were significantly lower in the TiQLB group (P < 0.001). A few cases of mild postoperative nausea and vomiting were noted among patients in both groups; however, the difference was not statistically significant. No incidence of pruritus, shivering, or respiratory depression was noted.
Conclusions: Analgesia after the ultrasound-guided TiQLB with bupivacaine was superior to that after the ultrasound-guided caudal block, with similar side effects.
Keywords: Analgesia; Bupivacaine; Interventional ultrasonography; Nerve block; Pediatrics; Postoperative pain..
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures
Similar articles
-
Dexmedetomidine Added to Bupivacaine versus Bupivacaine in Transincisional Ultrasound-Guided Quadratus Lumborum Block in Open Renal Surgeries: A Randomized Trial.Pain Physician. 2020 Jun;23(3):271-282. Pain Physician. 2020. PMID: 32517393 Clinical Trial.
-
Ultrasound-guided Techniques for Perioperative Analgesia in Pediatric Lower Abdominal Surgeries: Quadratus Lumborum Block with Bupivacaine versus Caudal Bupivacaine and Neostigmine.Pain Physician. 2023 Mar;26(2):137-147. Pain Physician. 2023. PMID: 36988360 Clinical Trial.
-
Ultrasound-Guided Techniques for Postoperative Analgesia in Patients Undergoing Laparoscopic Sleeve Gastrectomy: Erector Spinae Plane Block vs. Quadratus Lumborum Block.Pain Physician. 2023 May;26(3):245-256. Pain Physician. 2023. PMID: 37192227 Clinical Trial.
-
Ultrasound-guided quadratus lumborum block for postoperative analgesia in renal surgery: a systematic review and meta-analysis of randomized controlled trials.J Anesth. 2022 Apr;36(2):254-264. doi: 10.1007/s00540-022-03040-z. Epub 2022 Jan 22. J Anesth. 2022. PMID: 35064819
-
Ultrasound-guided quadratus lumborum block for postoperative analgesia: A systematic review and meta-analysis.Eur J Anaesthesiol. 2021 Feb 1;38(2):115-129. doi: 10.1097/EJA.0000000000001368. Eur J Anaesthesiol. 2021. PMID: 33186305
Cited by
-
Postoperative analgesic effects of the quadratus lumborum block in pediatric patients: a systematic review and meta-analysis.Korean J Pain. 2024 Jan 1;37(1):59-72. doi: 10.3344/kjp.23268. Epub 2023 Dec 21. Korean J Pain. 2024. PMID: 38123185 Free PMC article.
-
Pediatric fascial plane blocks: an educational review with technique, tips & tricks.BMC Anesthesiol. 2025 Jul 1;25(1):320. doi: 10.1186/s12871-025-03193-w. BMC Anesthesiol. 2025. PMID: 40596847 Free PMC article. Review.
-
The analgesic effects of quadratus lumborum block versus caudal block for pediatric patients undergoing abdominal surgery: a systematic review and meta-analysis.Front Pediatr. 2025 Feb 6;13:1492876. doi: 10.3389/fped.2025.1492876. eCollection 2025. Front Pediatr. 2025. PMID: 39981211 Free PMC article.
-
Fascial plane blocks in pediatric anesthesia: A narrative review.Saudi J Anaesth. 2025 Apr-Jun;19(2):190-197. doi: 10.4103/sja.sja_146_25. Epub 2025 Mar 25. Saudi J Anaesth. 2025. PMID: 40255350 Free PMC article. Review.
-
Quadratus lumborum block versus caudal block in paediatric surgeries: a protocol for systematic review and meta-analysis.BMJ Open. 2025 May 28;15(5):e100085. doi: 10.1136/bmjopen-2025-100085. BMJ Open. 2025. PMID: 40441771 Free PMC article.
References
-
- Piaggio L, Franc-Guimond J, Figueroa TE, Barthold JS, González R. Comparison of laparoscopic and open partial nephrectomy for duplication anomalies in children. J Urol. 2006;175:2269–73. - PubMed
-
- Klingler HC, Remzi M, Janetschek G, Kratzik C, Marberger MJ. Comparison of open versus laparoscopic pyeloplasty techniques in treatment of uretero-pelvic junction obstruction. Eur Urol. 2003;44:340–5. - PubMed
-
- Honeck P, Wendt-Nordahl G, Krombach P, Bach T, Häcker A, Alken P, et al. Does open stone surgery still play a role in the treatment of urolithiasis? Data of a primary urolithiasis center. J Endourol. 2009;23:1209–12. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
