

Readmissions and postdischarge mortality by race and ethnicity among Medicare beneficiaries with multimorbidity
- PMID: 36705464
- PMCID: PMC10258122
- DOI: 10.1111/jgs.18251
Readmissions and postdischarge mortality by race and ethnicity among Medicare beneficiaries with multimorbidity
Abstract
Background: Disparities in readmission risk and reasons they might exist among diverse complex patients with multimorbidity, disability, and unmet social needs have not been clearly established. These characteristics may be underestimated in claims-based studies where individual-level data are limited. We sought to examine the risk of readmissions and postdischarge mortality by race and ethnicity after rigorous adjustment for multimorbidity, physical functioning, and sociodemographic and lifestyle characteristics.
Methods: We used Health and Retirement Study (HRS) data linked to Medicare claims. To obtain ICD-9-CM diagnostic codes to compute the ICD-coded multimorbidity-weighted index (MWI-ICD) we used Medicare Parts A and B (inpatient, outpatient, carrier) files between 1991-2015. Participants must have had at least one hospitalization between January 1, 2000 and September 30, 2015 and continuous enrollment in fee-for-service Medicare Part A 1-year prior to hospitalization. We used multivariable logistic regression to assess the association of MWI-ICD with 30-day readmissions and mortality 1-year postdischarge. Using HRS data, we adjusted for age, sex, BMI, smoking, physical activity, education, household net worth, and living arrangement/marital status, and examined for effect modification by race and ethnicity.
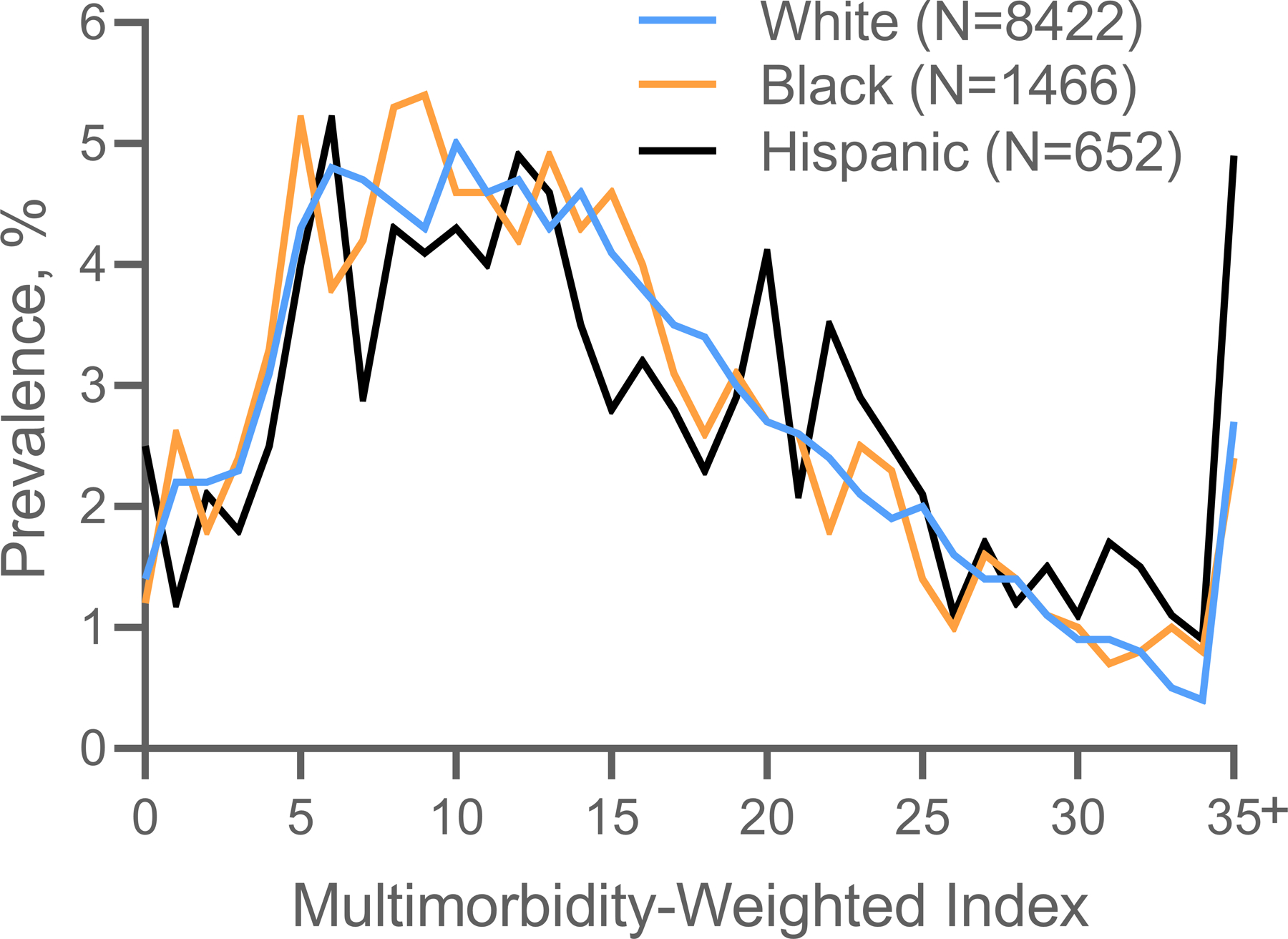
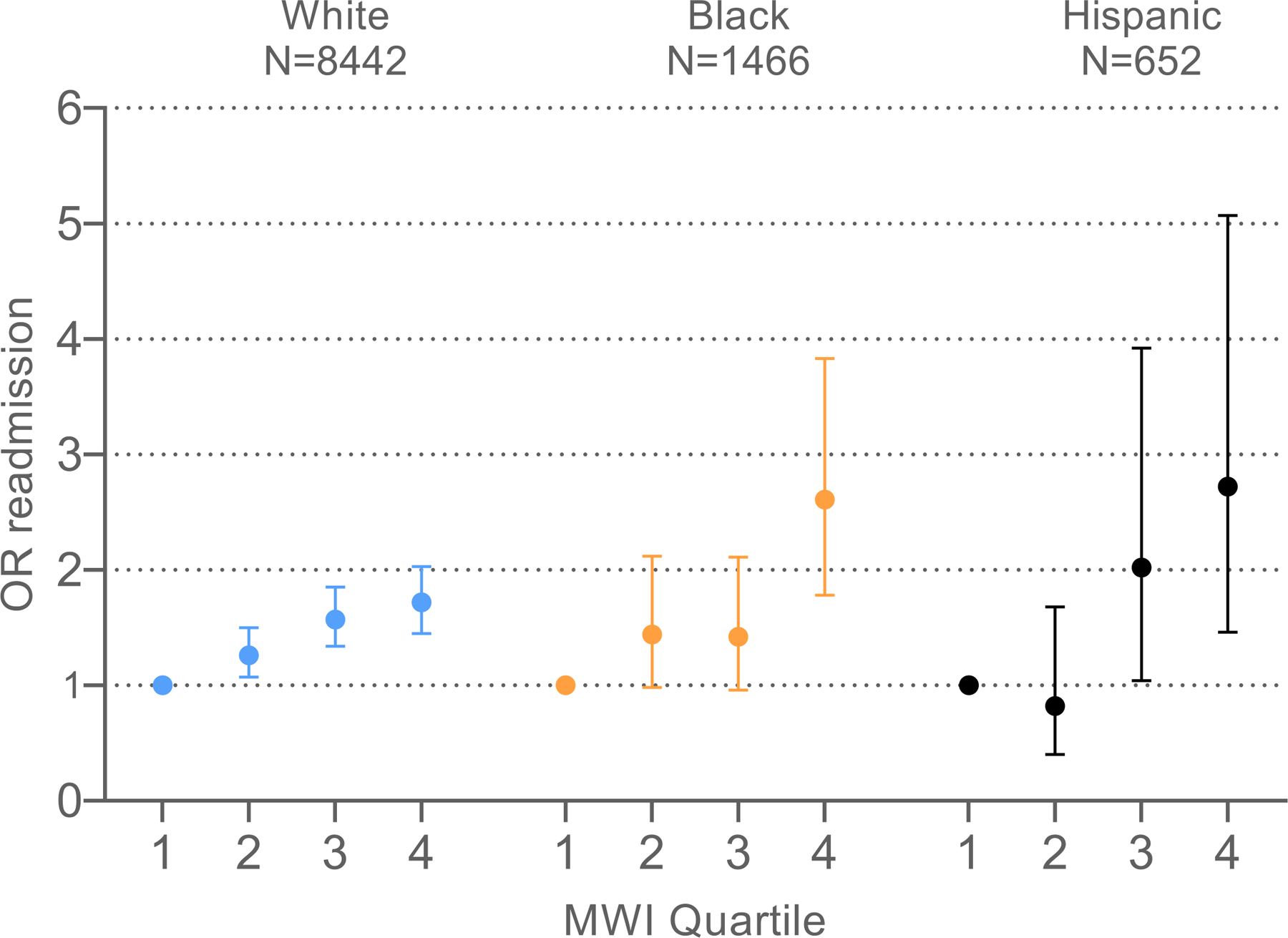
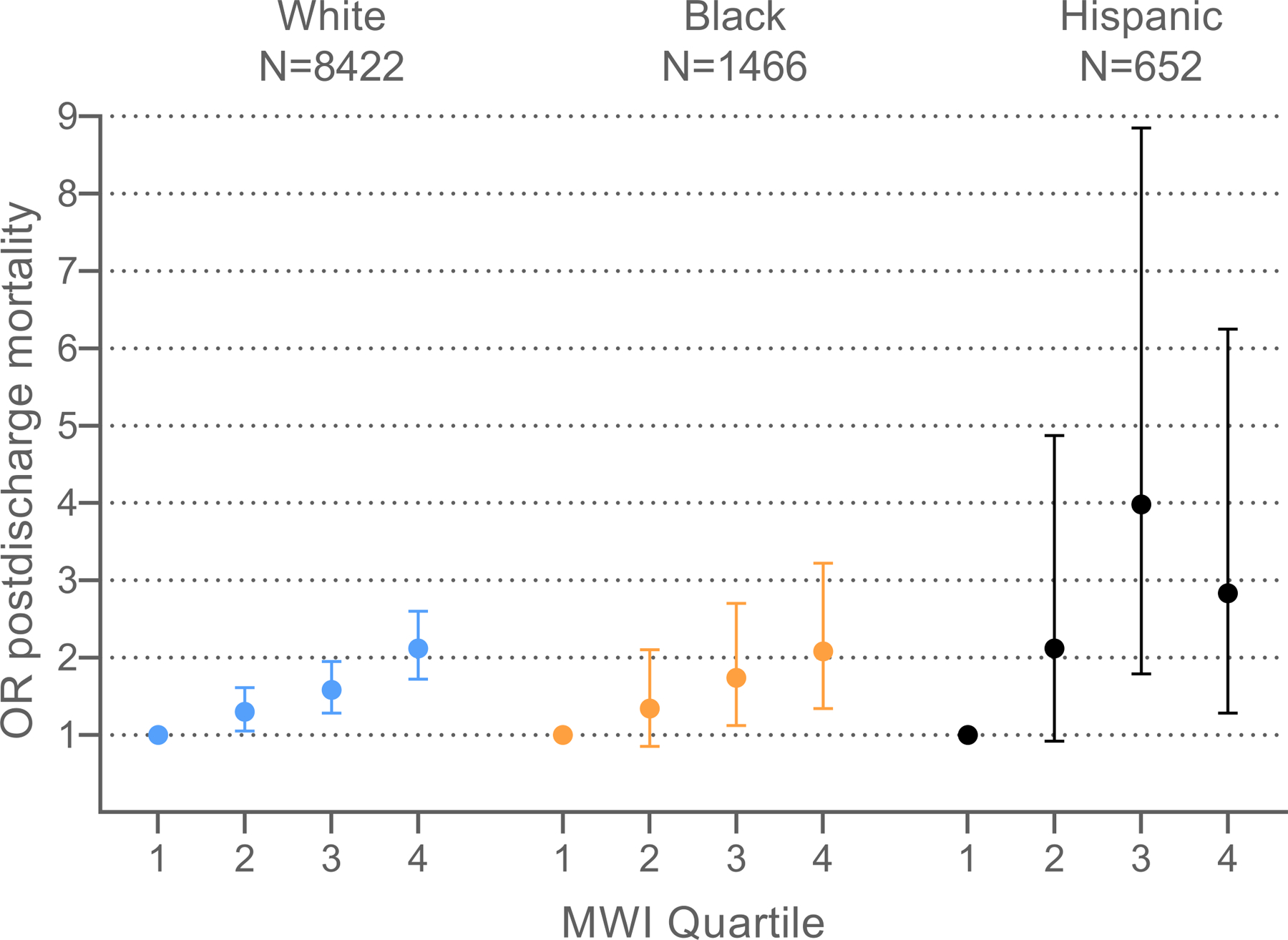
Results: The final sample of 10,737 participants had mean ± SD age 75.9 ± 8.7 years. Hispanic adults had the highest mean MWI-ICD (16.4 ± 10.1), followed by similar values for White (mean 14.8 ± 8.9) and Black (14.7 ± 8.9) adults. MWI-ICD was associated with a higher odds of readmission, and there was no significant effect modification by race and ethnicity. For postdischarge mortality, a 1-point increase MWI-ICD was associated with a 3% higher odds of mortality (OR = 1.03, 95% CI: 1.03-1.04), which did not significantly differ by race and ethnicity.
Conclusions: Multimorbidity was associated with a monotonic increased odds of 30-day readmission and 1-year postdischarge mortality across all race and ethnicity groups. There was no significant difference in readmission or mortality risk by race and ethnicity after robust adjustment.
Keywords: comorbidity; health disparities; hospital readmission; multiple chronic conditions.
© 2023 The American Geriatrics Society.
Conflict of interest statement
Figures
Similar articles
-
Multimorbidity, 30-Day Readmissions, and Postdischarge Mortality Among Medicare Beneficiaries Using a New ICD-Coded Multimorbidity-Weighted Index.J Gerontol A Biol Sci Med Sci. 2023 Mar 30;78(4):727-734. doi: 10.1093/gerona/glac242. J Gerontol A Biol Sci Med Sci. 2023. PMID: 36480692 Free PMC article.
-
Multimorbidity in Medicare Beneficiaries: Performance of an ICD-Coded Multimorbidity-Weighted Index.J Am Geriatr Soc. 2020 May;68(5):999-1006. doi: 10.1111/jgs.16310. Epub 2020 Jan 9. J Am Geriatr Soc. 2020. PMID: 31917465 Free PMC article.
-
Follow-up Post-discharge and Readmission Disparities Among Medicare Fee-for-Service Beneficiaries, 2018.J Gen Intern Med. 2022 Sep;37(12):3020-3028. doi: 10.1007/s11606-022-07488-3. J Gen Intern Med. 2022. PMID: 35355202 Free PMC article.
-
Association of Frailty With 30-Day Outcomes for Acute Myocardial Infarction, Heart Failure, and Pneumonia Among Elderly Adults.JAMA Cardiol. 2019 Nov 1;4(11):1084-1091. doi: 10.1001/jamacardio.2019.3511. JAMA Cardiol. 2019. PMID: 31553402 Free PMC article.
-
Disparities in 30-day readmission rates among Medicare enrollees with dementia.J Am Geriatr Soc. 2023 Jul;71(7):2194-2207. doi: 10.1111/jgs.18311. Epub 2023 Mar 10. J Am Geriatr Soc. 2023. PMID: 36896859 Free PMC article.
References
-
- Murray F, Allen M, Clark CM, Daly CJ, Jacobs DM. Socio-demographic and -economic factors associated with 30-day readmission for conditions targeted by the hospital readmissions reduction program: a population-based study. BMC Public Health 2021;21(1):1922. doi:10.1186/s12889-021-11987-z - DOI - PMC - PubMed
