

Efficacy and safety of metabolic interventions for the treatment of severe COVID-19: in vitro, observational, and non-randomized open-label interventional study
- PMID: 36705566
- PMCID: PMC9937660
- DOI: 10.7554/eLife.79946
Efficacy and safety of metabolic interventions for the treatment of severe COVID-19: in vitro, observational, and non-randomized open-label interventional study
Abstract
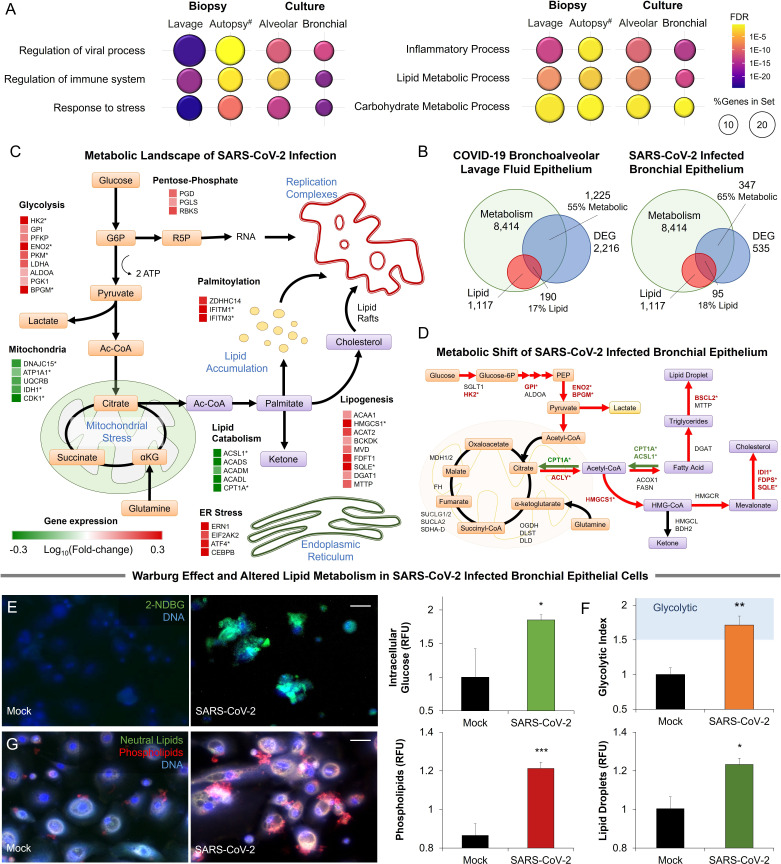
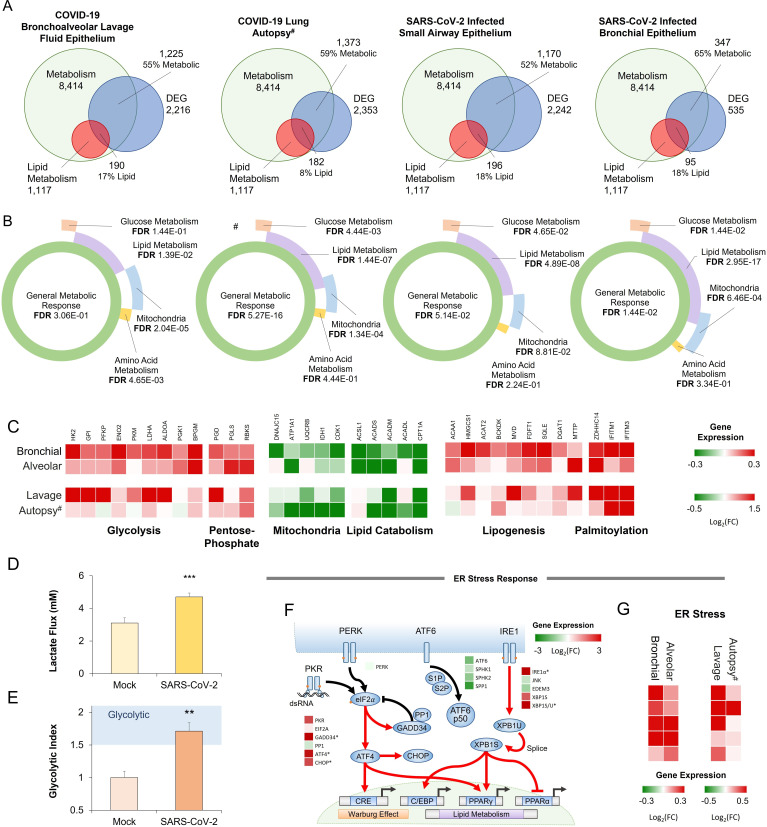
Background: Viral infection is associated with a significant rewire of the host metabolic pathways, presenting attractive metabolic targets for intervention.
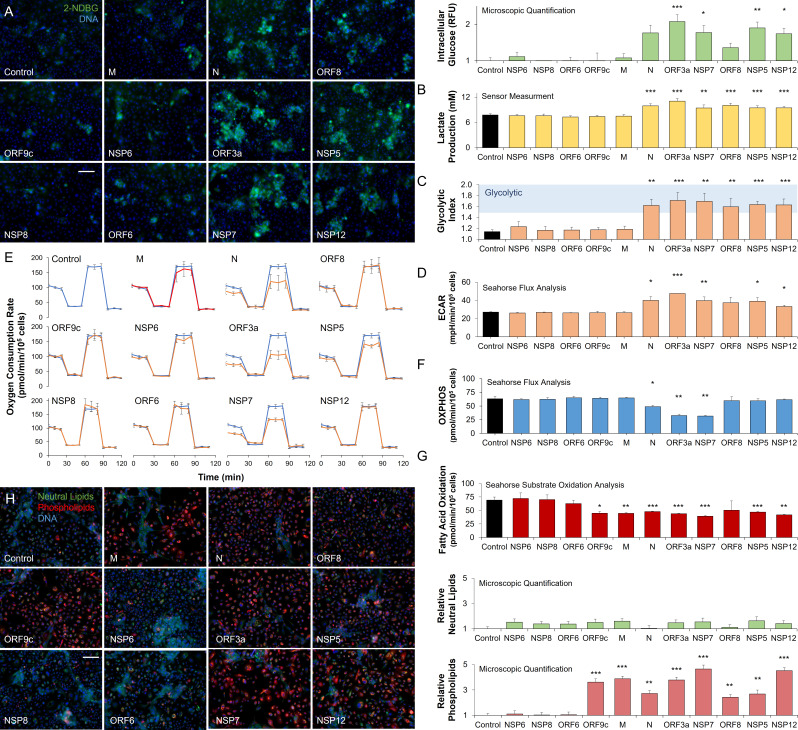
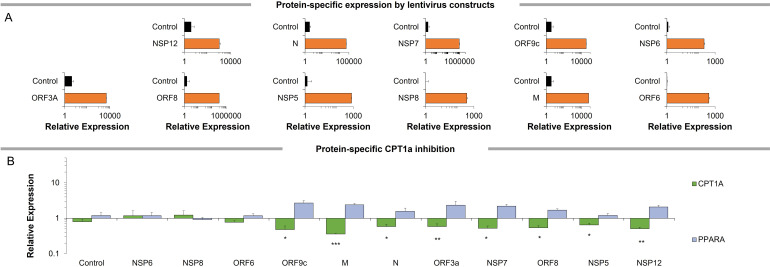
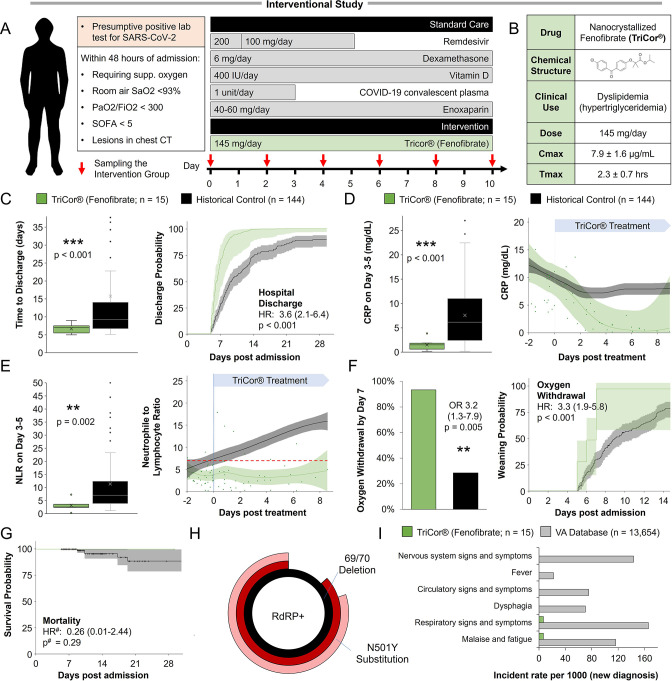
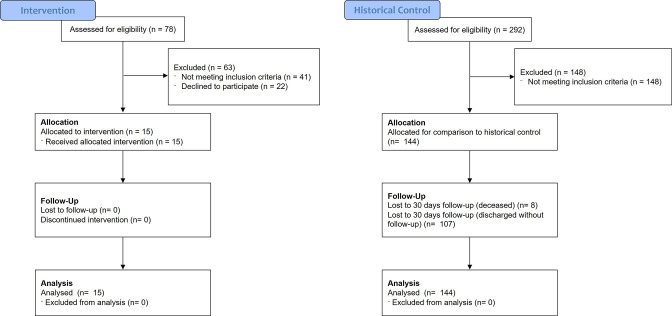
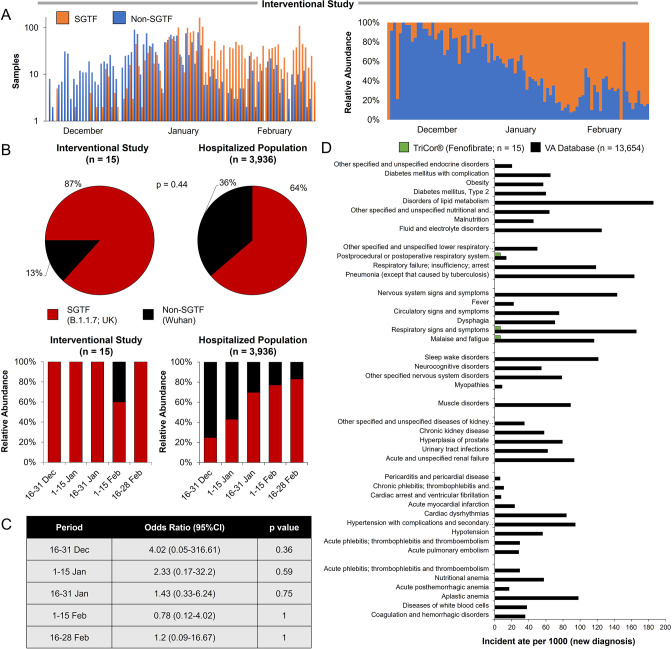
Methods: We chart the metabolic response of lung epithelial cells to SARS-CoV-2 infection in primary cultures and COVID-19 patient samples and perform in vitro metabolism-focused drug screen on primary lung epithelial cells infected with different strains of the virus. We perform observational analysis of Israeli patients hospitalized due to COVID-19 and comparative epidemiological analysis from cohorts in Italy and the Veteran's Health Administration in the United States. In addition, we perform a prospective non-randomized interventional open-label study in which 15 patients hospitalized with severe COVID-19 were given 145 mg/day of nanocrystallized fenofibrate added to the standard of care.
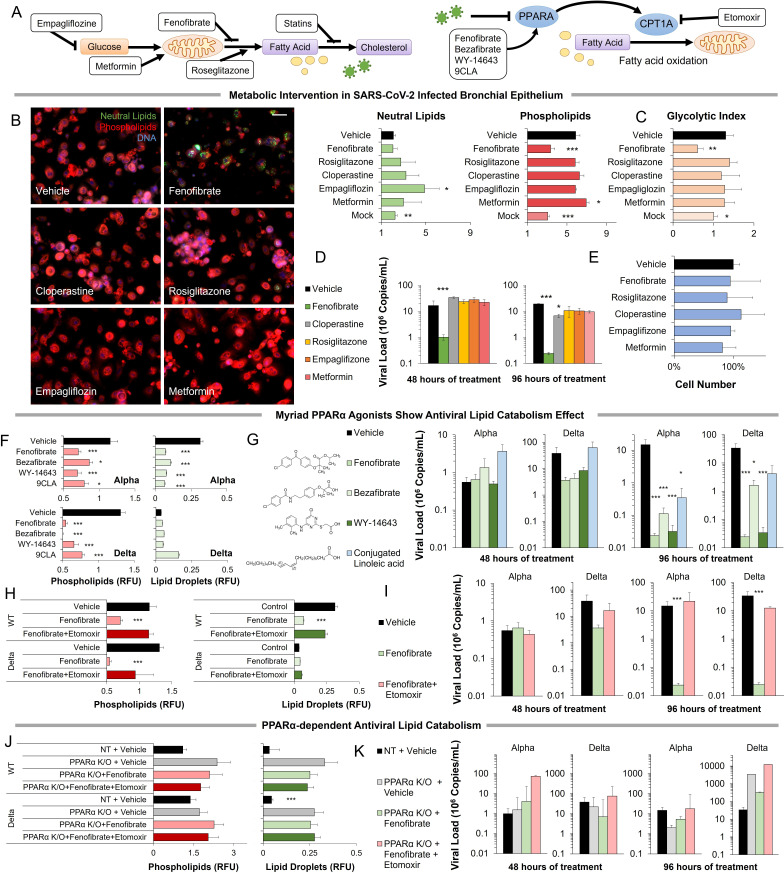
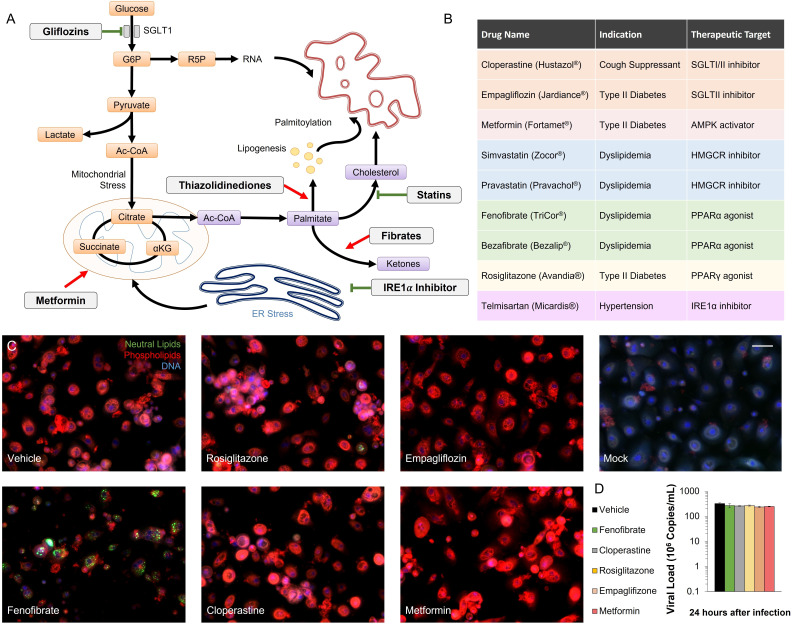
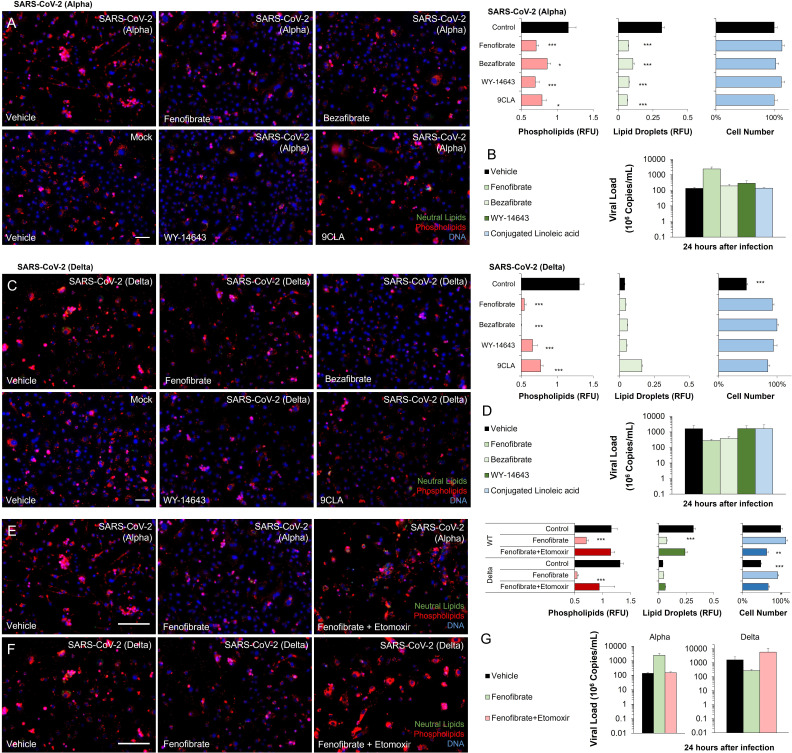
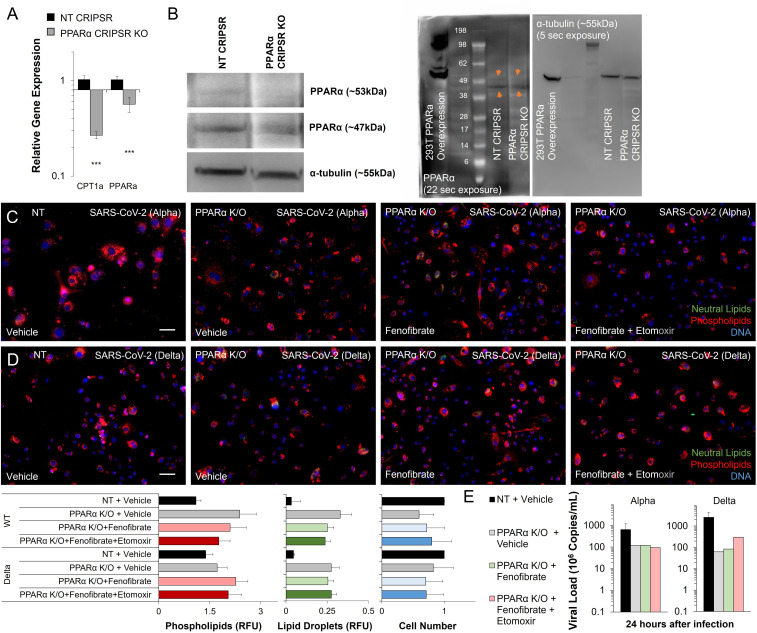
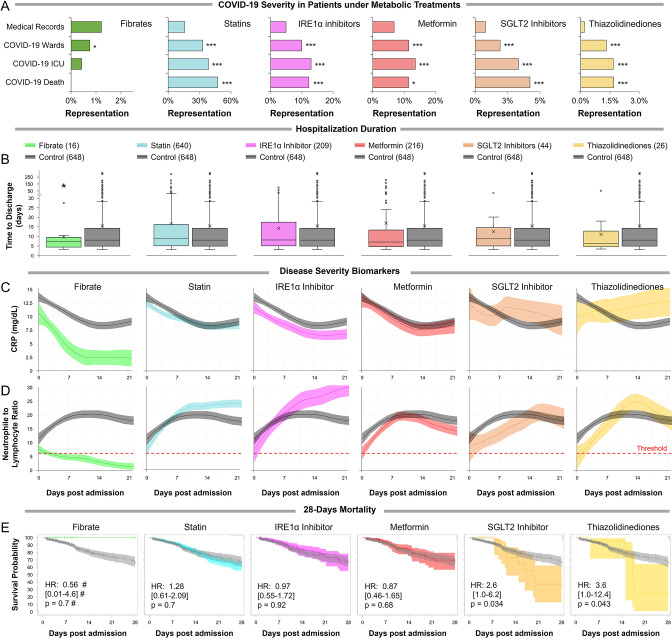
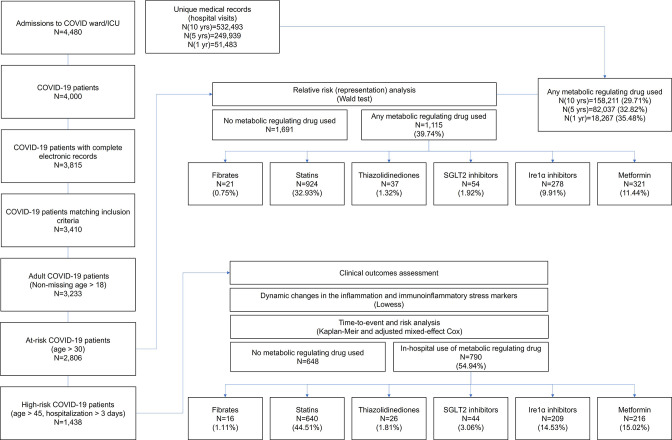
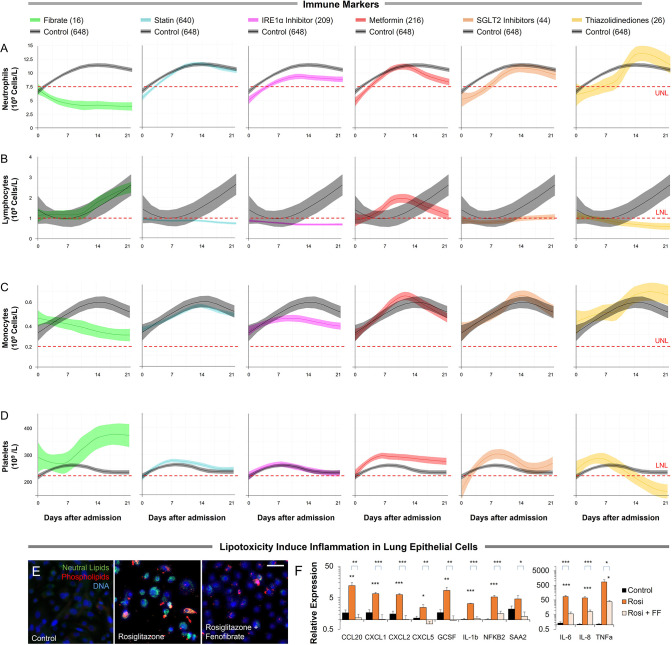
Results: SARS-CoV-2 infection produced transcriptional changes associated with increased glycolysis and lipid accumulation. Metabolism-focused drug screen showed that fenofibrate reversed lipid accumulation and blocked SARS-CoV-2 replication through a PPARα-dependent mechanism in both alpha and delta variants. Analysis of 3233 Israeli patients hospitalized due to COVID-19 supported in vitro findings. Patients taking fibrates showed significantly lower markers of immunoinflammation and faster recovery. Additional corroboration was received by comparative epidemiological analysis from cohorts in Europe and the United States. A subsequent prospective non-randomized interventional open-label study was carried out on 15 patients hospitalized with severe COVID-19. The patients were treated with 145 mg/day of nanocrystallized fenofibrate in addition to standard-of-care. Patients receiving fenofibrate demonstrated a rapid reduction in inflammation and a significantly faster recovery compared to patients admitted during the same period.
Conclusions: Taken together, our data suggest that pharmacological modulation of PPARα should be strongly considered as a potential therapeutic approach for SARS-CoV-2 infection and emphasizes the need to complete the study of fenofibrate in large randomized controlled clinical trials.
Funding: Funding was provided by European Research Council Consolidator Grants OCLD (project no. 681870) and generous gifts from the Nikoh Foundation and the Sam and Rina Frankel Foundation (YN). The interventional study was supported by Abbott (project FENOC0003).
Clinical trial number: NCT04661930.
Keywords: COVID-19; cell biology; drug repurposing; medicine; metabolic regulation; translational research; viruses.
© 2023, Ehrlich et al.
Conflict of interest statement
AE is registered as an investor in a PCT regarding the use of metabolic regulators for COVID. The author has a patent on the use of PPAR agonists to treat COVID. The author has no other competing interests to declare, KI, MN, IA, YD, NA, LK, NR, MH, SS, IH, CP, MC, AG, AB, MM, SM No competing interests declared, AC has received personal honoraria for statistical consultation from Recipharm, and personal honoraria for manuscript writing from both Sharper Srl and Fidia Pharmaceuticals. The author has no other competing interests to declare, CS is President of Fondazione (totally supported by family). The author has no other competing interests to declare, JC received funding from National Institutes of Health (1R01HL157108-01A1,1R01AG074989-01) . The author has no other competing interests to declare, JC has received consulting honoraria from Sanifit, Bristol Myers Squibb, Merck, Edwards Lifesciences, Bayer, JNJ, Fukuda-Denshi, NGM Bio, Mayo institute of technology and the University of Delaware, and research grants from the National Institutes of Health, Abbott, Microsoft, Fukuda-Denshi and Bristol Myers Squibb. He has received compensation from the American Heart Association and the American College of Cardiology for editorial roles, and visiting speaker honoraria from Washington University, Emory University, University of Utah, the Japanese Association for Cardiovascular Nursing and the Korean Society of Cardiology. The author is named as inventor in a University of Pennsylvania patent for the use of inorganic nitrates/nitrites for the treatment of Heart Failure and Preserved Ejection Fraction and for the use of biomarkers in heart failure with preserved ejection fraction. The author has participated on the Advisory board for Bristol-Myers Squibb Data safety monitoring board for studies by the University of Delaware and UT Southwestern, and is Vice President of North American Artery Society. The author has received research device loans from Atcor Medical, Fukuda-Denshi, Unex, Uscom, NDD Medical Technologies, Microsoft, and MicroVision Medical. The author has no other competing interests to declare, LD is affiliated with BioStats Statistical Consulting Ltd where they work as a Biostatistician. The authors has received payment for statistical work for the manuscript and consulting fees from Tissue Dynamics Ltd. The author has no other competing interests to declare, OS has received consulting honoraria from Sanofi, Roche and Neopharm, and lectures honoraria from Roche . He is the chairmen of the Israel Association for the study of the liver. The author has no other competing interests to declare, YN is registered as an investor in a PCT regarding the use of metabolic regulators for COVID and has a patent on the use of PPAR agonists to treat COVID. The author has no other competing interests to declare
Figures
Similar articles
-
Safety and Efficacy of Imatinib for Hospitalized Adults with COVID-19: A structured summary of a study protocol for a randomised controlled trial.Trials. 2020 Oct 28;21(1):897. doi: 10.1186/s13063-020-04819-9. Trials. 2020. PMID: 33115543 Free PMC article.
-
Virtualized clinical studies to assess the natural history and impact of gut microbiome modulation in non-hospitalized patients with mild to moderate COVID-19 a randomized, open-label, prospective study with a parallel group study evaluating the physiologic effects of KB109 on gut microbiota structure and function: a structured summary of a study protocol for a randomized controlled study.Trials. 2021 Apr 2;22(1):245. doi: 10.1186/s13063-021-05157-0. Trials. 2021. PMID: 33810796 Free PMC article.
-
PROTECT Trial: A cluster-randomized study with hydroxychloroquine versus observational support for prevention or early-phase treatment of Coronavirus disease (COVID-19): A structured summary of a study protocol for a randomized controlled trial.Trials. 2020 Jul 31;21(1):689. doi: 10.1186/s13063-020-04527-4. Trials. 2020. PMID: 32736597 Free PMC article.
-
Ivermectin for preventing and treating COVID-19.Cochrane Database Syst Rev. 2021 Jul 28;7(7):CD015017. doi: 10.1002/14651858.CD015017.pub2. Cochrane Database Syst Rev. 2021. Update in: Cochrane Database Syst Rev. 2022 Jun 21;6:CD015017. doi: 10.1002/14651858.CD015017.pub3. PMID: 34318930 Free PMC article. Updated.
-
Fenofibrate for COVID-19 and related complications as an approach to improve treatment outcomes: the missed key for Holy Grail.Inflamm Res. 2022 Nov;71(10-11):1159-1167. doi: 10.1007/s00011-022-01615-w. Epub 2022 Aug 8. Inflamm Res. 2022. PMID: 35941297 Free PMC article. Review.
Cited by
-
Long Neuro-COVID-19: Current Mechanistic Views and Therapeutic Perspectives.Biomolecules. 2024 Aug 28;14(9):1081. doi: 10.3390/biom14091081. Biomolecules. 2024. PMID: 39334847 Free PMC article. Review.
-
Mitochondria and the Repurposing of Diabetes Drugs for Off-Label Health Benefits.Int J Mol Sci. 2025 Jan 3;26(1):364. doi: 10.3390/ijms26010364. Int J Mol Sci. 2025. PMID: 39796218 Free PMC article. Review.
-
Antiviral Activity Against SARS-CoV-2 Variants Using in Silico and in Vitro Approaches.J Microbiol. 2023 Jul;61(7):703-711. doi: 10.1007/s12275-023-00062-4. Epub 2023 Jun 26. J Microbiol. 2023. PMID: 37358709
-
Diabetes Mellitus, Energy Metabolism, and COVID-19.Endocr Rev. 2024 Mar 4;45(2):281-308. doi: 10.1210/endrev/bnad032. Endocr Rev. 2024. PMID: 37934800 Free PMC article. Review.
References
-
- Ajaz S, McPhail MJ, Singh KK, Mujib S, Trovato FM, Napoli S, Agarwal K. Mitochondrial metabolic manipulation by SARS-cov-2 in peripheral blood mononuclear cells of patients with COVID-19. American Journal of Physiology. Cell Physiology. 2021;320:C57–C65. doi: 10.1152/ajpcell.00426.2020. - DOI - PMC - PubMed
-
- Akter F, Mannan A, Mehedi HMH, Rob MA, Ahmed S, Salauddin A, Hossain MS, Hasan MM. Clinical characteristics and short term outcomes after recovery from COVID-19 in patients with and without diabetes in bangladesh. Diabetes & Metabolic Syndrome. 2020;14:2031–2038. doi: 10.1016/j.dsx.2020.10.016. - DOI - PMC - PubMed
-
- Ali MS, Prieto-Alhambra D, Lopes LC, Ramos D, Bispo N, Ichihara MY, Pescarini JM, Williamson E, Fiaccone RL, Barreto ML, Smeeth L. Propensity score methods in health technology assessment: principles, extended applications, and recent advances. Frontiers in Pharmacology. 2019;10:973. doi: 10.3389/fphar.2019.00973. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
Associated data
- Actions
- Actions
- Actions
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
