

Efficient representations of binarized health deficit data: the frailty index and beyond
- PMID: 36705846
- PMCID: PMC10400752
- DOI: 10.1007/s11357-022-00723-z
Efficient representations of binarized health deficit data: the frailty index and beyond
Abstract
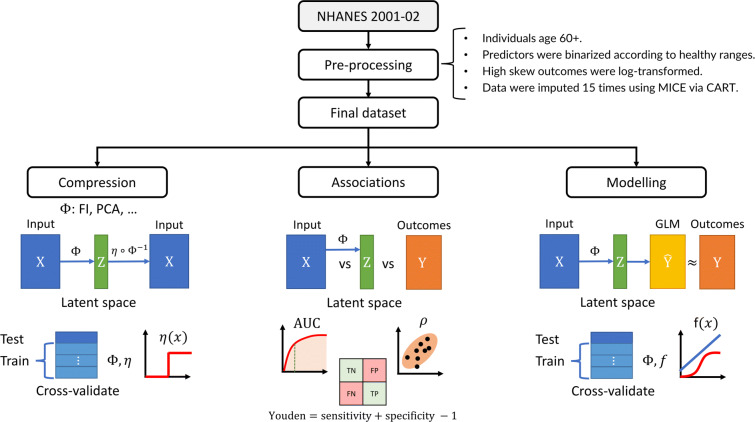
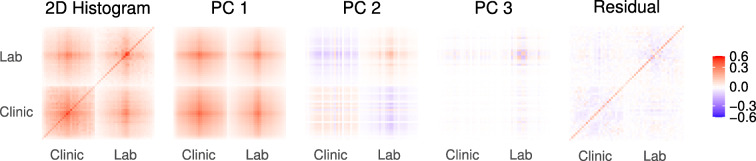
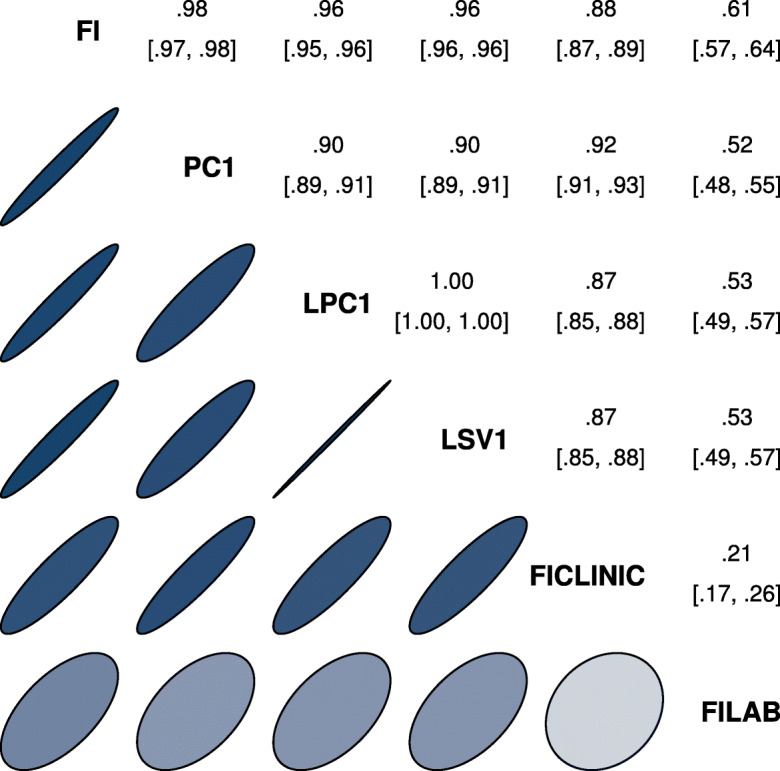
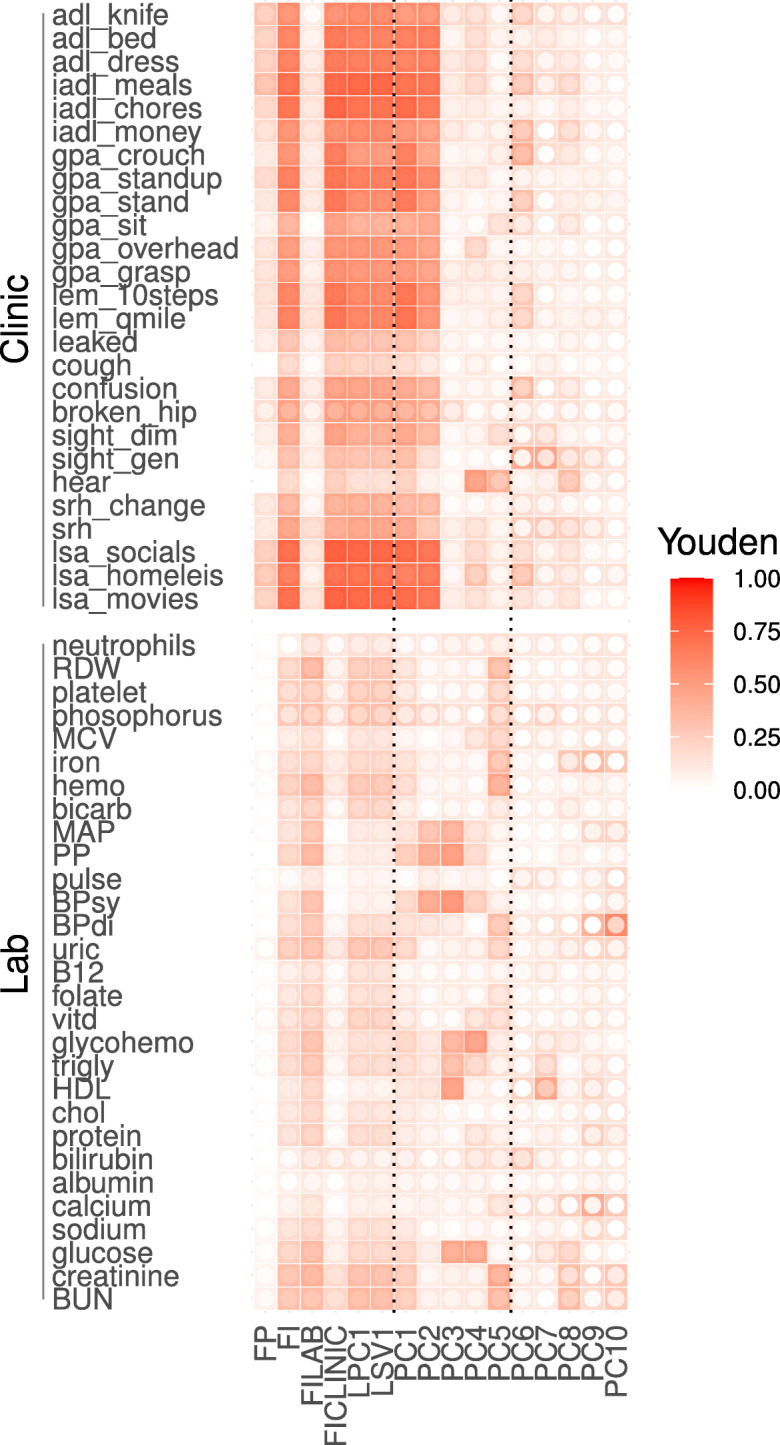
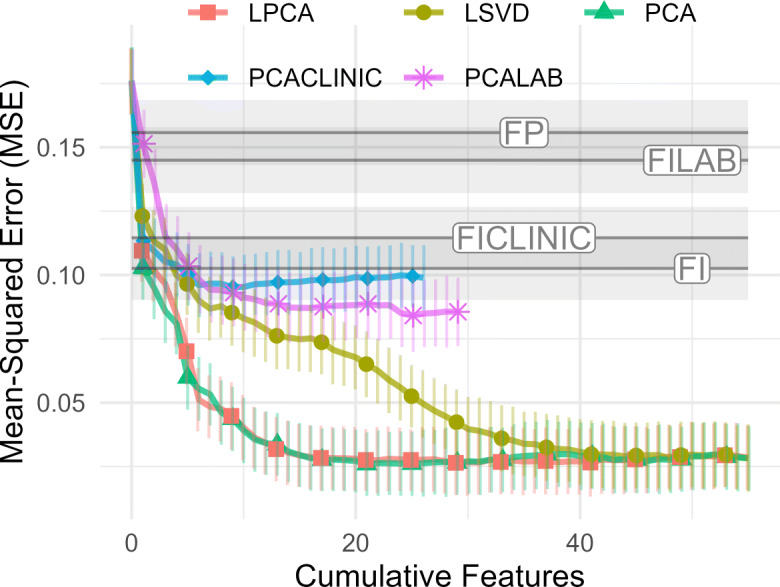
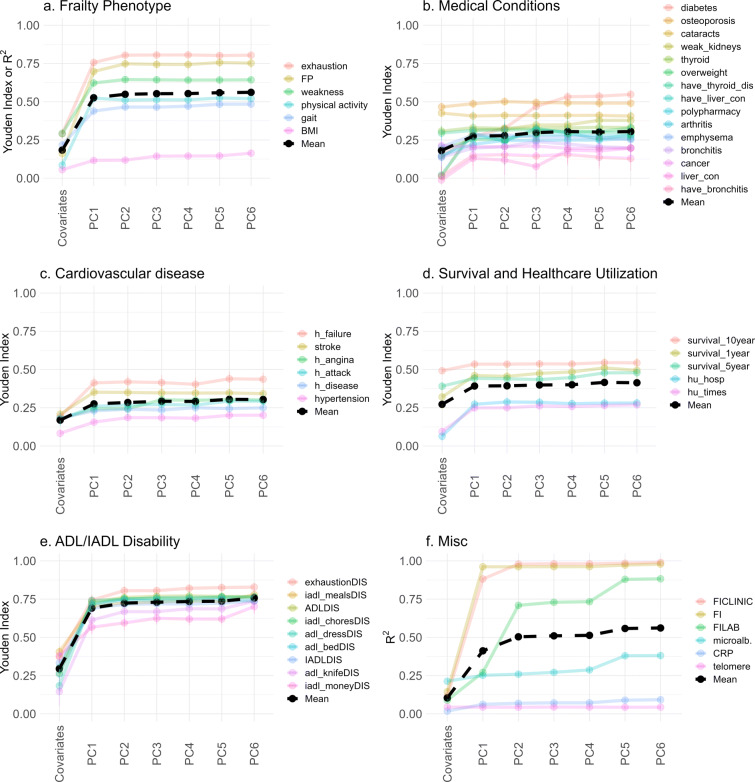
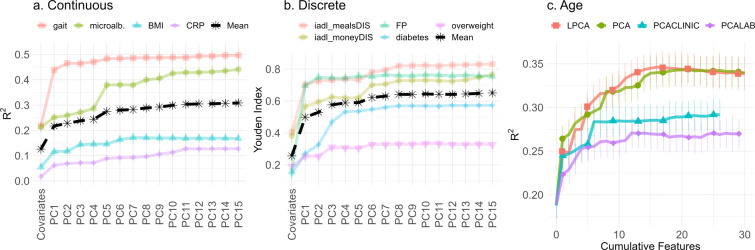
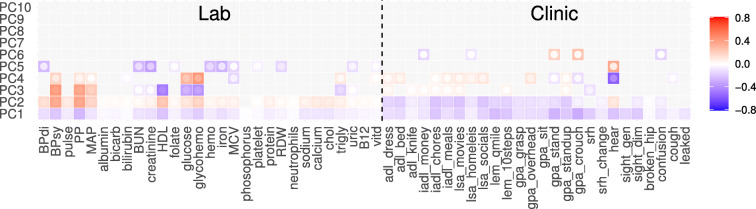
We investigated efficient representations of binarized health deficit data using the 2001-2002 National Health and Nutrition Examination Survey (NHANES). We compared the abilities of features to compress health deficit data and to predict adverse outcomes. We used principal component analysis (PCA) and several other dimensionality reduction techniques, together with several varieties of the frailty index (FI). We observed that the FI approximates the first - primary - component obtained by PCA and other compression techniques. Most adverse outcomes were well predicted using only the FI. While the FI is therefore a useful technique for compressing binary deficits into a single variable, additional dimensions were needed for high-fidelity compression of health deficit data. Moreover, some outcomes - including inflammation and metabolic dysfunction - showed high-dimensional behaviour. We generally found that clinical data were easier to compress than lab data. Our results help to explain the success of the FI as a simple dimensionality reduction technique for binary health data. We demonstrate how PCA extends the FI, providing additional health information, and allows us to explore system dimensionality and complexity. PCA is a promising tool for determining and exploring collective health features from collections of binarized biomarkers.
Keywords: Aging; Biological age; Dimensionality reduction; Frailty index; Logistic principal component analysis; Principal component analysis.
© 2023. The Author(s), under exclusive licence to American Aging Association.
Figures




Similar articles
-
Informative frailty indices from binarized biomarkers.Biogerontology. 2020 Jun;21(3):345-355. doi: 10.1007/s10522-020-09863-1. Epub 2020 Mar 10. Biogerontology. 2020. PMID: 32157458
-
A frailty index from common clinical and laboratory tests predicts increased risk of death across the life course.Geroscience. 2017 Aug;39(4):447-455. doi: 10.1007/s11357-017-9993-7. Epub 2017 Sep 2. Geroscience. 2017. PMID: 28866737 Free PMC article.
-
The association between frailty, the metabolic syndrome, and mortality over the lifespan.Geroscience. 2017 Apr;39(2):221-229. doi: 10.1007/s11357-017-9967-9. Epub 2017 Mar 9. Geroscience. 2017. PMID: 28281219 Free PMC article.
-
Implementation of the mouse frailty index.Can J Physiol Pharmacol. 2017 Oct;95(10):1149-1155. doi: 10.1139/cjpp-2017-0025. Epub 2017 May 2. Can J Physiol Pharmacol. 2017. PMID: 28463656 Review.
-
Frailty Index as a clinical measure of biological age in psychiatry.J Affect Disord. 2020 May 1;268:183-187. doi: 10.1016/j.jad.2020.03.015. Epub 2020 Mar 6. J Affect Disord. 2020. PMID: 32174476 Review.
Cited by
-
Principal component-based clinical aging clocks identify signatures of healthy aging and targets for clinical intervention.Nat Aging. 2024 Aug;4(8):1137-1152. doi: 10.1038/s43587-024-00646-8. Epub 2024 Jun 19. Nat Aging. 2024. PMID: 38898237 Free PMC article.
-
Wealth gradients in healthy aging: evidence from the 2011 and 2013 waves of the China Health and Retirement Longitudinal Study.Arch Public Health. 2025 Feb 21;83(1):47. doi: 10.1186/s13690-025-01526-2. Arch Public Health. 2025. PMID: 39985065 Free PMC article.
-
Network dynamical stability analysis reveals key "mallostatic" natural variables that erode homeostasis and drive age-related decline of health.Sci Rep. 2023 Dec 13;13(1):22140. doi: 10.1038/s41598-023-49129-7. Sci Rep. 2023. PMID: 38092834 Free PMC article.
-
Explainable machine learning framework for biomarker discovery by combining biological age and frailty prediction.Sci Rep. 2025 Apr 22;15(1):13924. doi: 10.1038/s41598-025-98948-3. Sci Rep. 2025. PMID: 40263505 Free PMC article.
-
Dynamical Network Stability Analysis of Multiple Biological Ages Provides a Framework for Understanding the Aging Process.J Gerontol A Biol Sci Med Sci. 2024 Oct 1;79(10):glae021. doi: 10.1093/gerona/glae021. J Gerontol A Biol Sci Med Sci. 2024. PMID: 38206765 Free PMC article.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous
