

ReachCare Mobile Apps for Patients Experiencing Suicidality in the Emergency Department: Development and Usability Testing Using Mixed Methods
- PMID: 36705961
- PMCID: PMC9919536
- DOI: 10.2196/41422
ReachCare Mobile Apps for Patients Experiencing Suicidality in the Emergency Department: Development and Usability Testing Using Mixed Methods
Abstract
Background: Many individuals with suicide risk present to acute care settings such as emergency departments (EDs). However, staffing and time constraints mean that many EDs are not well equipped to deliver evidence-based interventions for patients experiencing suicidality. An existing intervention initiated in the ED for patients with suicide risk (Emergency Department Safety Assessment and Follow-up Evaluation [ED-SAFE]) has been found to be effective but faces trenchant barriers for widespread adoption.
Objective: On the basis of the ED-SAFE intervention, we aimed to develop 2 apps for patients with suicide risk: a web app guiding patients through safety planning in the ED (ED app) and a smartphone app providing patients components of the ED-SAFE program on their phones after discharge (patient app). We then tested the usability of these apps with patients presenting to the ED with suicide risk.
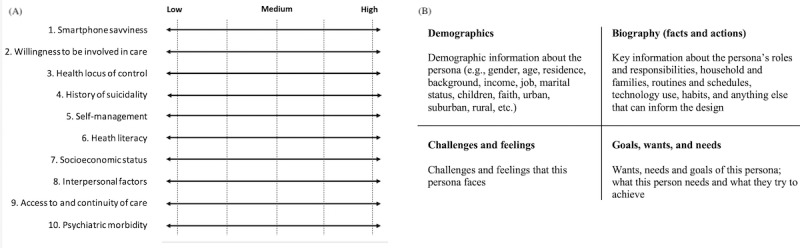
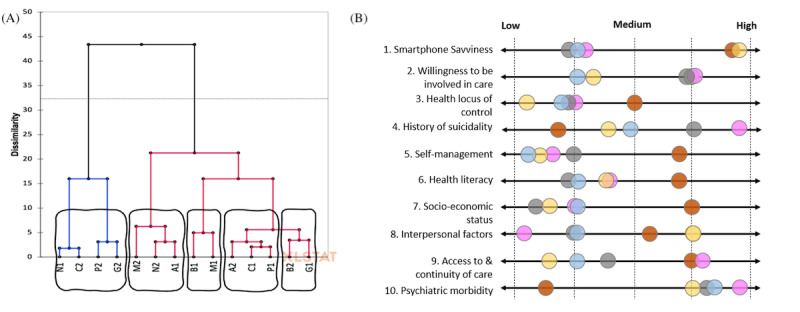
Methods: Using a user-centered design framework, we first developed user personas to explore the needs and characteristics of patients who are at risk for suicide using inputs from clinicians (n=3) and suicidologists (n=4). Next, we validated these personas during interviews with individuals with lived experience of suicidality (n=6) and used them to inform our application designs. We field-tested the apps with ED patients presenting with suicide risk (n=14) in 2 iterative cycles to assess their usability and engagement using a mixed methods approach. We also rated the quality and fidelity of the safety plans created.
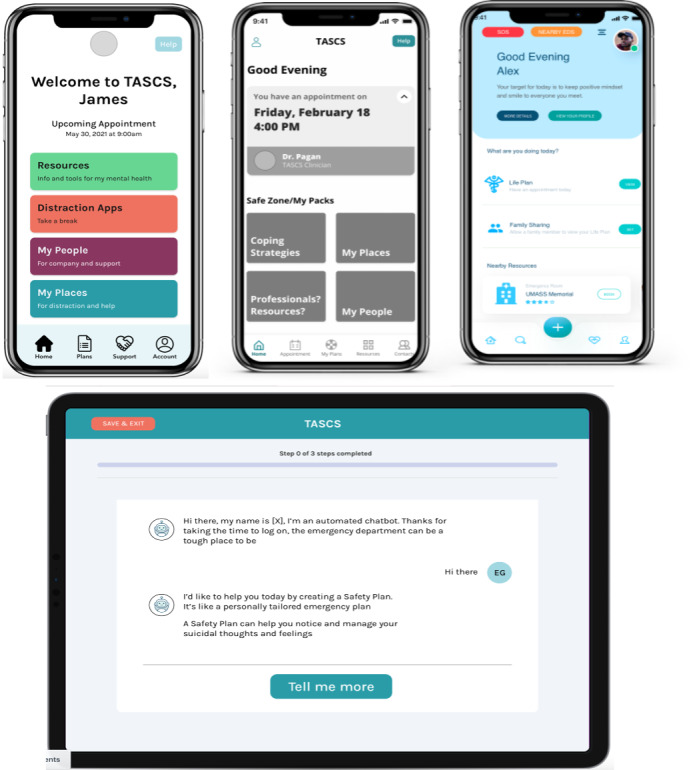
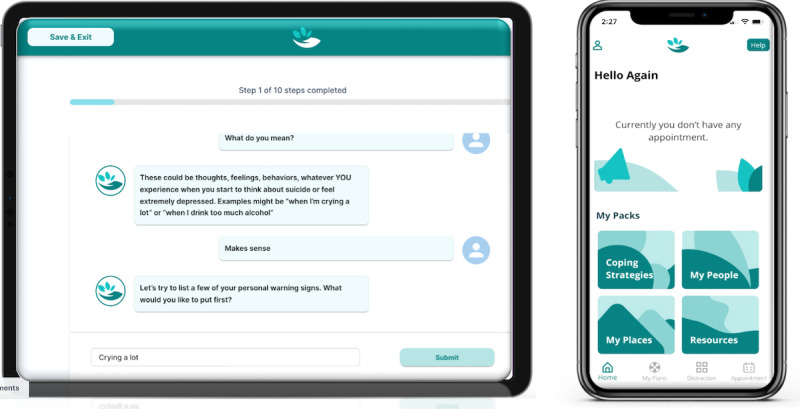
Results: We developed 2 interoperable and complementary apps. The first is a web app designed for use on a tablet device during ED admission that guides the patient by creating a safety plan using a chatbot-style interface. The second is a smartphone app for use after discharge and allows the patient to view, edit, and share their completed safety plan; access self-care education, helplines, and behavioral health referrals; and track follow-up appointments with the study clinician. The initial prototype usability testing (n=9) demonstrated satisfactory scores (ED app System Usability Scale [SUS], mean 78.6/100, SD 24.1; User Engagement Scale, mean 3.74/5, SD 0.72; patient app SUS, mean 81.7/100, SD 20.1). After refining the apps based on participant feedback, the second cycle testing (n=5) showed improvement (ED app SUS, mean 90.5/100, SD 9.9; User Engagement Scale, mean 4.07/5, SD 0.36; patient app SUS, mean 97.0/100, SD 1.9). The quality ratings for completed safety plans were satisfactory (Safety Planning Intervention Scoring Algorithm-Brief, mean 27.4, SD 3.4).
Conclusions: By adopting a user-centered approach and creating personas to guide development, we were able to create apps for ED patients with suicide risk and obtain satisfactory usability, engagement, and quality scores. Developing digital health tools based on user-centered design principles that deliver evidence-based intervention components may help overcome trenchant implementation barriers in challenging health care settings.
Keywords: emergency department; engagement; mobile app; mobile phone; suicide; usability.
©Celine Larkin, Soussan Djamasbi, Edwin D Boudreaux, Fatima Varzgani, Roscoe Garner, Mariam Siddique, John Pietro, Bengisu Tulu. Originally published in JMIR Formative Research (https://formative.jmir.org), 27.01.2023.
Conflict of interest statement
Conflicts of Interest: None declared.
Figures
Similar articles
-
Translating Suicide Safety Planning Components Into the Design of mHealth App Features: Systematic Review.JMIR Ment Health. 2024 Mar 28;11:e52763. doi: 10.2196/52763. JMIR Ment Health. 2024. PMID: 38546711 Free PMC article.
-
Comparing the Acceptability and Quality of Intervention Modalities for Suicidality in the Emergency Department: Randomized Feasibility Trial.JMIR Ment Health. 2023 Oct 24;10:e49783. doi: 10.2196/49783. JMIR Ment Health. 2023. PMID: 37874619 Free PMC article.
-
Popular Evidence-Based Commercial Mental Health Apps: Analysis of Engagement, Functionality, Aesthetics, and Information Quality.JMIR Mhealth Uhealth. 2021 Jul 14;9(7):e29689. doi: 10.2196/29689. JMIR Mhealth Uhealth. 2021. PMID: 34259639 Free PMC article.
-
Development of a Smartphone App to Predict and Improve the Rates of Suicidal Ideation Among Transgender Persons (TransLife): Qualitative Study.J Med Internet Res. 2021 Mar 24;23(3):e24023. doi: 10.2196/24023. J Med Internet Res. 2021. PMID: 33596181 Free PMC article.
-
Review and Comparative Evaluation of Mobile Apps for Cardiovascular Risk Estimation: Usability Evaluation Using mHealth App Usability Questionnaire.JMIR Mhealth Uhealth. 2025 May 8;13:e56466. doi: 10.2196/56466. JMIR Mhealth Uhealth. 2025. PMID: 40341099 Free PMC article. Review.
Cited by
-
Digital Interventions for Adolescents and Young Adults Experiencing Self-Injurious Thoughts and Behaviors.Curr Treat Options Psychiatry. 2024 Jun;11(2):76-89. doi: 10.1007/s40501-024-00318-9. Epub 2024 Apr 24. Curr Treat Options Psychiatry. 2024. PMID: 39525358 Free PMC article.
-
Translating Suicide Safety Planning Components Into the Design of mHealth App Features: Systematic Review.JMIR Ment Health. 2024 Mar 28;11:e52763. doi: 10.2196/52763. JMIR Ment Health. 2024. PMID: 38546711 Free PMC article.
-
Digital therapeutics in the hospital for suicide crisis - content and design recommendations from young people and hospital staff.Digit Health. 2024 Feb 14;10:20552076241230072. doi: 10.1177/20552076241230072. eCollection 2024 Jan-Dec. Digit Health. 2024. PMID: 38362237 Free PMC article.
-
Comparing the Acceptability and Quality of Intervention Modalities for Suicidality in the Emergency Department: Randomized Feasibility Trial.JMIR Ment Health. 2023 Oct 24;10:e49783. doi: 10.2196/49783. JMIR Ment Health. 2023. PMID: 37874619 Free PMC article.
-
A Suicide Prevention Digital Technology for Individuals Experiencing an Acute Suicide Crisis in Emergency Departments: Naturalistic Observational Study of Real-World Acceptability, Feasibility, and Safety.JMIR Form Res. 2024 Sep 16;8:e52293. doi: 10.2196/52293. JMIR Form Res. 2024. PMID: 39283664 Free PMC article.
References
-
- Heron M. Deaths: leading causes for 2019. Natl Vital Stat Rep. 2021 Jul;70(9):1–114. doi: 10.15620/cdc:104186. http://www.cdc.gov/nchs/data/nvsr/nvsr70/nvsr70-09-508.pdf - DOI - PubMed
-
- Murphy SL, Xu J, Kochanek KD, Arias E. Mortality in the United States, 2017. NCHS Data Brief. 2018 Nov;(328):1–8. doi: 10.3886/icpsr07632. http://www.cdc.gov/nchs/data/databriefs/db328-h.pdf - DOI - PubMed
-
- Owens PL, McDermott KW, Lipari RN, Hambrick MM. Healthcare Cost and Utilization Project (HCUP) Statistical Briefs. Rockville, MD, USA: Agency for Healthcare Research and Quality; 2020. Emergency Department Visits Related to Suicidal Ideation or Suicide Attempt, 2008–2017. - PubMed
-
- Ahmedani BK, Simon GE, Stewart C, Beck A, Waitzfelder BE, Rossom R, Lynch F, Owen-Smith A, Hunkeler EM, Whiteside U, Operskalski BH, Coffey MJ, Solberg LI. Health care contacts in the year before suicide death. J Gen Intern Med. 2014 Jun;29(6):870–7. doi: 10.1007/s11606-014-2767-3. https://europepmc.org/abstract/MED/24567199 - DOI - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
