

Evaluating and mitigating bias in machine learning models for cardiovascular disease prediction
- PMID: 36706849
- PMCID: PMC11104322
- DOI: 10.1016/j.jbi.2023.104294
Evaluating and mitigating bias in machine learning models for cardiovascular disease prediction
Abstract
Objective: The study aims to investigate whether machine learning-based predictive models for cardiovascular disease (CVD) risk assessment show equivalent performance across demographic groups (such as race and gender) and if bias mitigation methods can reduce any bias present in the models. This is important as systematic bias may be introduced when collecting and preprocessing health data, which could affect the performance of the models on certain demographic sub-cohorts. The study is to investigate this using electronic health records data and various machine learning models.
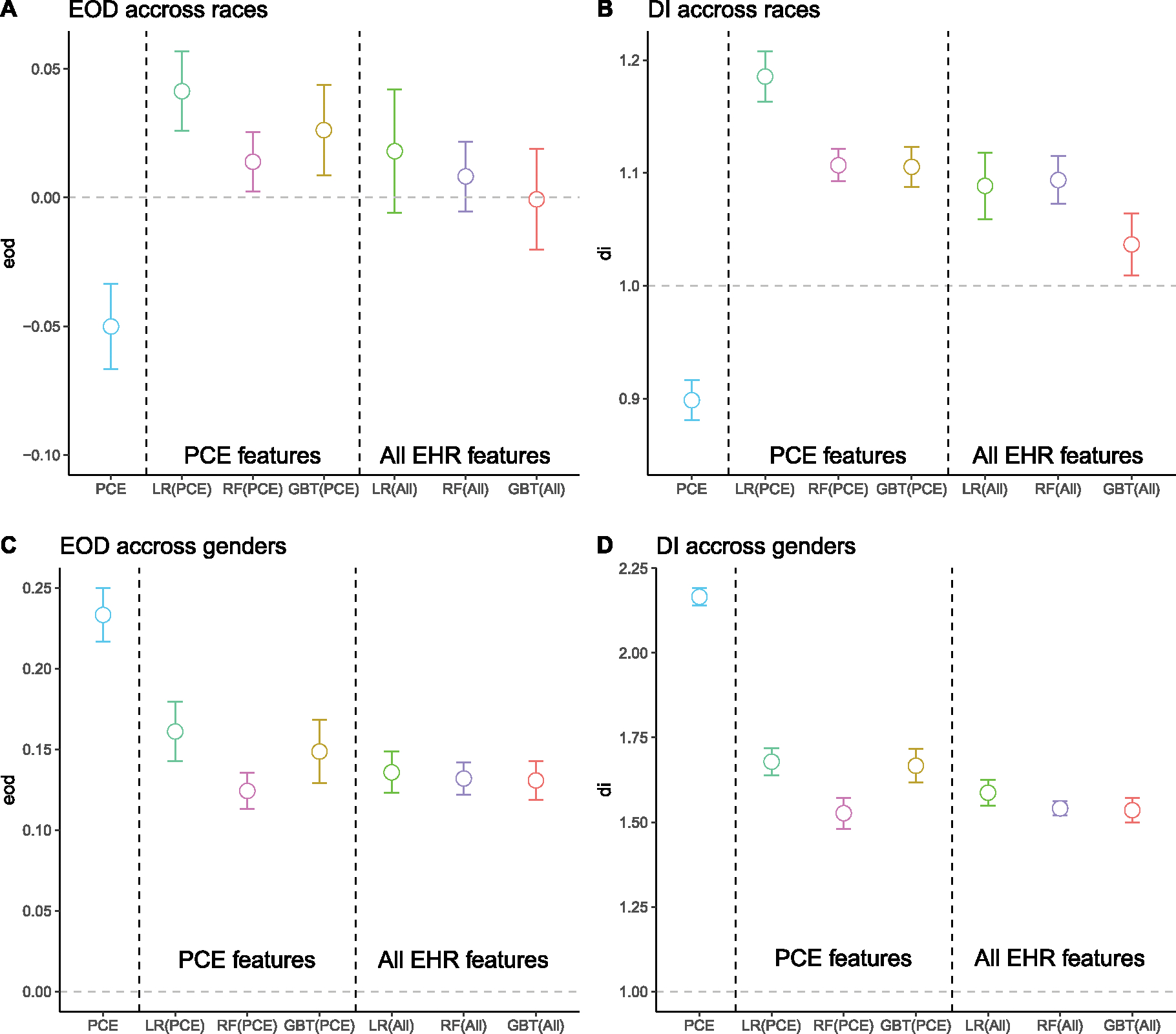
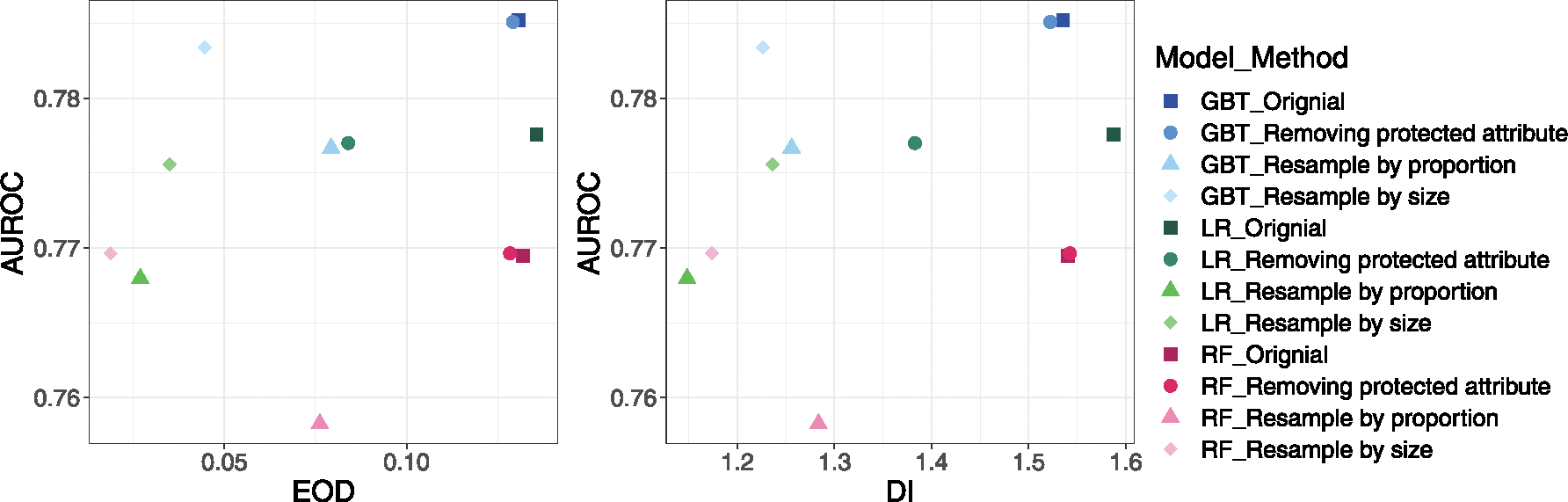
Methods: The study used large de-identified Electronic Health Records data from Vanderbilt University Medical Center. Machine learning (ML) algorithms including logistic regression, random forest, gradient-boosting trees, and long short-term memory were applied to build multiple predictive models. Model bias and fairness were evaluated using equal opportunity difference (EOD, 0 indicates fairness) and disparate impact (DI, 1 indicates fairness). In our study, we also evaluated the fairness of a non-ML baseline model, the American Heart Association (AHA) Pooled Cohort Risk Equations (PCEs). Moreover, we compared the performance of three different de-biasing methods: removing protected attributes (e.g., race and gender), resampling the imbalanced training dataset by sample size, and resampling by the proportion of people with CVD outcomes.
Results: The study cohort included 109,490 individuals (mean [SD] age 47.4 [14.7] years; 64.5% female; 86.3% White; 13.7% Black). The experimental results suggested that most ML models had smaller EOD and DI than PCEs. For ML models, the mean EOD ranged from -0.001 to 0.018 and the mean DI ranged from 1.037 to 1.094 across race groups. There was a larger EOD and DI across gender groups, with EOD ranging from 0.131 to 0.136 and DI ranging from 1.535 to 1.587. For debiasing methods, removing protected attributes didn't significantly reduced the bias for most ML models. Resampling by sample size also didn't consistently decrease bias. Resampling by case proportion reduced the EOD and DI for gender groups but slightly reduced accuracy in many cases.
Conclusions: Among the VUMC cohort, both PCEs and ML models were biased against women, suggesting the need to investigate and correct gender disparities in CVD risk prediction. Resampling by proportion reduced the bias for gender groups but not for race groups.
Keywords: Bias mitigation; Cardiovascular diseases; Clinical predictive models; Electronic health records; Fairness; Machine learning.
Copyright © 2023 Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of Competing Interest The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures

Similar articles
-
Comparison of Methods to Reduce Bias From Clinical Prediction Models of Postpartum Depression.JAMA Netw Open. 2021 Apr 1;4(4):e213909. doi: 10.1001/jamanetworkopen.2021.3909. JAMA Netw Open. 2021. PMID: 33856478 Free PMC article.
-
Fairness in Predicting Cancer Mortality Across Racial Subgroups.JAMA Netw Open. 2024 Jul 1;7(7):e2421290. doi: 10.1001/jamanetworkopen.2024.21290. JAMA Netw Open. 2024. PMID: 38985468 Free PMC article.
-
Predictive Accuracy of Stroke Risk Prediction Models Across Black and White Race, Sex, and Age Groups.JAMA. 2023 Jan 24;329(4):306-317. doi: 10.1001/jama.2022.24683. JAMA. 2023. PMID: 36692561 Free PMC article.
-
Folic acid supplementation and malaria susceptibility and severity among people taking antifolate antimalarial drugs in endemic areas.Cochrane Database Syst Rev. 2022 Feb 1;2(2022):CD014217. doi: 10.1002/14651858.CD014217. Cochrane Database Syst Rev. 2022. PMID: 36321557 Free PMC article.
-
Evaluation and Mitigation of Racial Bias in Clinical Machine Learning Models: Scoping Review.JMIR Med Inform. 2022 May 31;10(5):e36388. doi: 10.2196/36388. JMIR Med Inform. 2022. PMID: 35639450 Free PMC article.
Cited by
-
Computational strategic recruitment for representation and coverage studied in the All of Us Research Program.NPJ Digit Med. 2025 Jul 3;8(1):402. doi: 10.1038/s41746-025-01804-x. NPJ Digit Med. 2025. PMID: 40610586 Free PMC article.
-
Architectural Design of a Blockchain-Enabled, Federated Learning Platform for Algorithmic Fairness in Predictive Health Care: Design Science Study.J Med Internet Res. 2023 Oct 30;25:e46547. doi: 10.2196/46547. J Med Internet Res. 2023. PMID: 37902833 Free PMC article.
-
Machine Learning and Bias in Medical Imaging: Opportunities and Challenges.Circ Cardiovasc Imaging. 2024 Feb;17(2):e015495. doi: 10.1161/CIRCIMAGING.123.015495. Epub 2024 Feb 20. Circ Cardiovasc Imaging. 2024. PMID: 38377237 Free PMC article. Review.
-
Large Language Models for Wearable Sensor-Based Human Activity Recognition, Health Monitoring, and Behavioral Modeling: A Survey of Early Trends, Datasets, and Challenges.Sensors (Basel). 2024 Aug 4;24(15):5045. doi: 10.3390/s24155045. Sensors (Basel). 2024. PMID: 39124092 Free PMC article. Review.
-
Machine learning based prediction models for cardiovascular disease risk using electronic health records data: systematic review and meta-analysis.Eur Heart J Digit Health. 2024 Oct 27;6(1):7-22. doi: 10.1093/ehjdh/ztae080. eCollection 2025 Jan. Eur Heart J Digit Health. 2024. PMID: 39846062 Free PMC article. Review.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
