

Artificial intelligence reveals features associated with breast cancer neoadjuvant chemotherapy responses from multi-stain histopathologic images
- PMID: 36707660
- PMCID: PMC9883475
- DOI: 10.1038/s41698-023-00352-5
Artificial intelligence reveals features associated with breast cancer neoadjuvant chemotherapy responses from multi-stain histopathologic images
Abstract
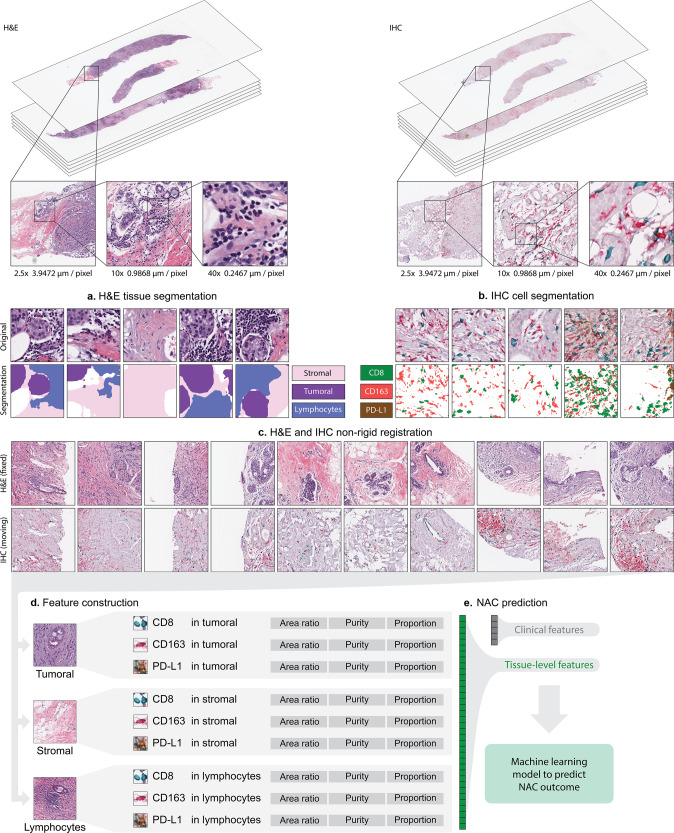
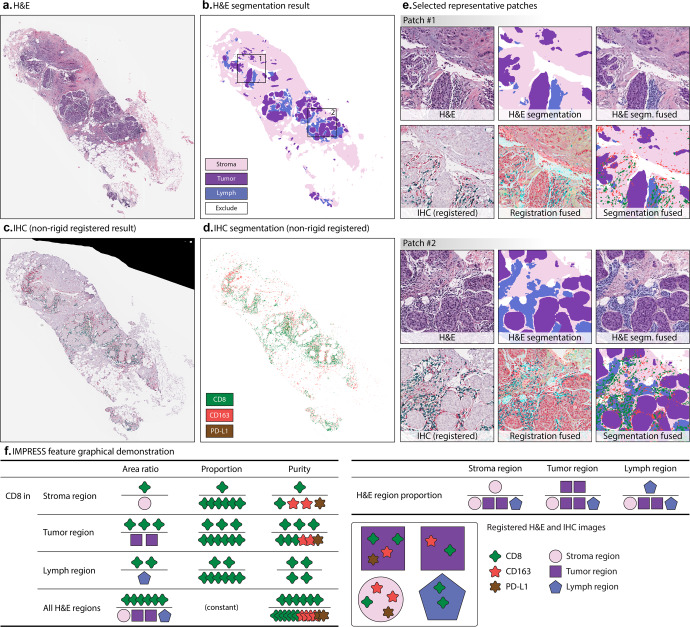
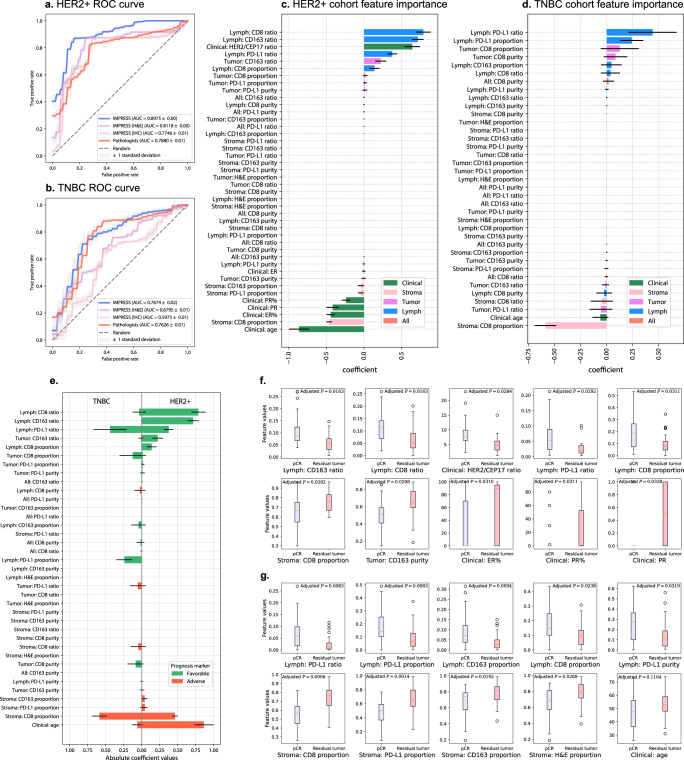
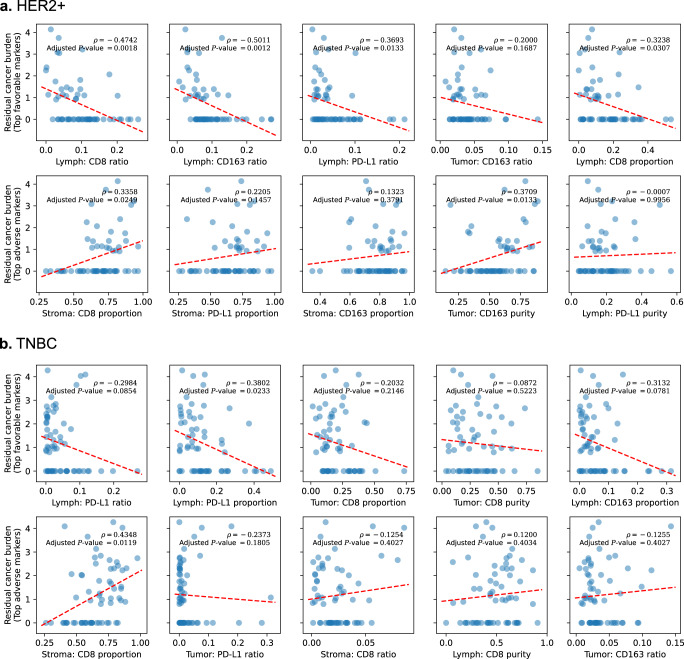
Advances in computational algorithms and tools have made the prediction of cancer patient outcomes using computational pathology feasible. However, predicting clinical outcomes from pre-treatment histopathologic images remains a challenging task, limited by the poor understanding of tumor immune micro-environments. In this study, an automatic, accurate, comprehensive, interpretable, and reproducible whole slide image (WSI) feature extraction pipeline known as, IMage-based Pathological REgistration and Segmentation Statistics (IMPRESS), is described. We used both H&E and multiplex IHC (PD-L1, CD8+, and CD163+) images, investigated whether artificial intelligence (AI)-based algorithms using automatic feature extraction methods can predict neoadjuvant chemotherapy (NAC) outcomes in HER2-positive (HER2+) and triple-negative breast cancer (TNBC) patients. Features are derived from tumor immune micro-environment and clinical data and used to train machine learning models to accurately predict the response to NAC in breast cancer patients (HER2+ AUC = 0.8975; TNBC AUC = 0.7674). The results demonstrate that this method outperforms the results trained from features that were manually generated by pathologists. The developed image features and algorithms were further externally validated by independent cohorts, yielding encouraging results, especially for the HER2+ subtype.
© 2023. The Author(s).
Conflict of interest statement
H.N. is an employee of Roche Diagnostic Inc. All other authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
