

Establishment and evaluation of nomogram for predicting intraventricular hemorrhage in neonatal acute respiratory distress syndrome
- PMID: 36707776
- PMCID: PMC9883912
- DOI: 10.1186/s12887-023-03853-1
Establishment and evaluation of nomogram for predicting intraventricular hemorrhage in neonatal acute respiratory distress syndrome
Abstract
Background: Intraventricular hemorrhage (IVH) is the most common type of brain injury in newborns, especially in newborns with Neonatal acute respiratory distress syndrome (ARDS). IVH can cause brain parenchyma damage and long-term neurological sequelae in children. Early identification and prevention of sequelae are essential. This study aims to establish a predictive nomogram for the early prediction of IVH in newborns with ARDS.
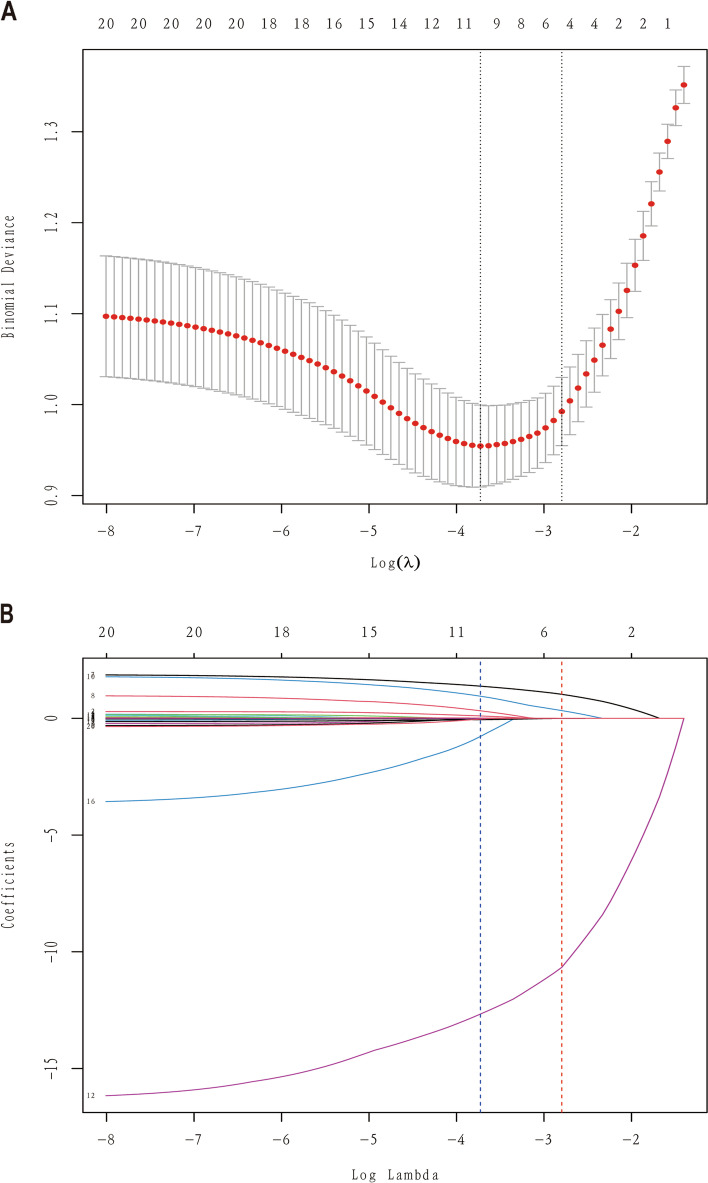
Methods: From 2019 to 2021, we collected data from 222 infants diagnosed with ARDS in the Department of Neonatology, First Affiliated Hospital of Xinjiang Medical University. Infants have been randomly assigned to the training set (n = 161) or the validation set (n = 61) at a ratio of 7:3. Variables were screened using the Least Absolute Contract and Selection Operator (LASSO) regression to create a risk model for IVH in infants with ARDS. The variables chosen in the LASSO regression model were used to establish the prediction model using multivariate logistic regression analysis.
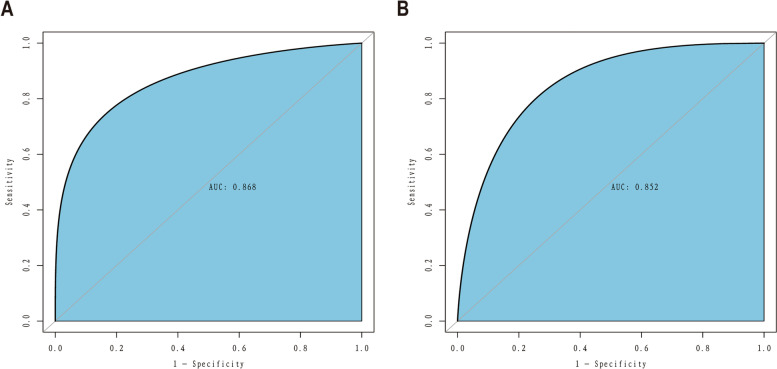
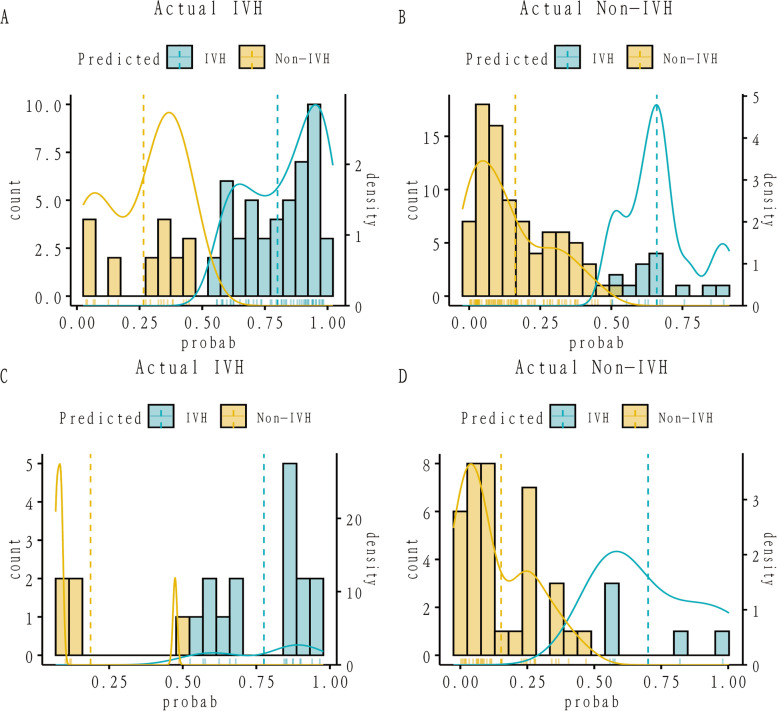
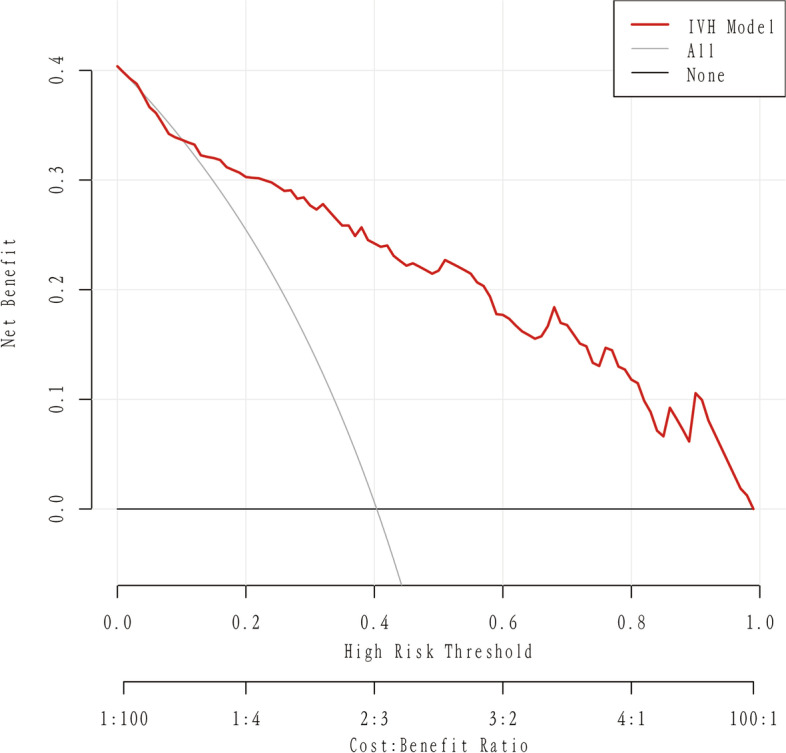
Results: We recognized 4 variables as independent risk factors for IVH in newborns with ARDS via LASSO analysis, consisting of premature rupture of membranes (PROM), pulmonary surfactant (PS) dosage, PH1 and Arterial partial pressure of oxygen (PaO21). The C-Index for this dataset is 0.868 (95% CI: 0.837-0.940) and the C index in bootstrap verification is 0.852 respectively. The analysis of the decision curve shows that the model can significantly improve clinical efficiency in predicting IVH. We also provide a website based on the model and open it to users for free, so that the model can be better applied to clinical practice.
Conclusion: In conclusion, the nomogram based on 4 factors shows good identification, calibration and clinical practicability. Our nomographs can help clinicians make clinical decisions, screen high-risk ARDS newborns, and facilitate early identification and management of IVH patients.
Keywords: Intraventricular hemorrhage (IVH); Neonatal acute respiratory distress syndrome (ARDS); Nomogram; Prediction model; Risk factors.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that there are no competing interests regarding the publication of this paper.
Figures




Similar articles
-
[Establishment of a predictive nomogram model for predicting the death of very preterm infants during hospitalization].Zhongguo Dang Dai Er Ke Za Zhi. 2022 Jun 15;24(6):654-661. doi: 10.7499/j.issn.1008-8830.2202027. Zhongguo Dang Dai Er Ke Za Zhi. 2022. PMID: 35762432 Free PMC article. Clinical Trial. Chinese.
-
Establishment and evaluation of nomogram for predicting acute respiratory distress syndrome in meconium-stained amniotic fluid neonates.Pediatr Pulmonol. 2025 Jan;60(1):e27345. doi: 10.1002/ppul.27345. Epub 2024 Nov 27. Pediatr Pulmonol. 2025. PMID: 39601453
-
Establishment and validation of apnea risk prediction models in preterm infants: a retrospective case control study.BMC Pediatr. 2024 Oct 11;24(1):654. doi: 10.1186/s12887-024-05125-y. BMC Pediatr. 2024. PMID: 39394551 Free PMC article.
-
Intraventricular hemorrhage and long-term outcome in the premature infant.J Neurosci Nurs. 1997 Oct;29(5):281-9. doi: 10.1097/01376517-199710000-00002. J Neurosci Nurs. 1997. PMID: 9361998 Review.
-
Intraventricular Hemorrhage in Premature Infants: A Historical Review.World Neurosurg. 2021 Sep;153:21-25. doi: 10.1016/j.wneu.2021.06.043. Epub 2021 Jun 16. World Neurosurg. 2021. PMID: 34144164 Review.
Cited by
-
Risk factors for brain injury in premature infants with twin-to-twin transfusion syndrome: a retrospective cohort study.Transl Pediatr. 2023 Dec 26;12(12):2121-2130. doi: 10.21037/tp-23-387. Epub 2023 Dec 19. Transl Pediatr. 2023. PMID: 38197096 Free PMC article.
-
A nomogram for predicting neonatal acute respiratory distress syndrome in patients with neonatal pneumonia after 34 weeks of gestation.Front Pediatr. 2025 Jan 9;12:1451466. doi: 10.3389/fped.2024.1451466. eCollection 2024. Front Pediatr. 2025. PMID: 39850203 Free PMC article.
-
Do Different Amounts of Exogenous Surfactant Differently Influence Cerebrovascular Instability in a Consecutive Group of Preterm Babies? Preliminary Results from a Single-Center Experience.Children (Basel). 2024 Sep 5;11(9):1088. doi: 10.3390/children11091088. Children (Basel). 2024. PMID: 39334621 Free PMC article.
-
Construction and evaluation of neonatal respiratory failure risk prediction model for neonatal respiratory distress syndrome.BMC Pulm Med. 2024 Jan 2;24(1):8. doi: 10.1186/s12890-023-02819-4. BMC Pulm Med. 2024. PMID: 38166798 Free PMC article. Clinical Trial.
-
Development of a machine learning model to identify intraventricular hemorrhage using time-series analysis in preterm infants.Sci Rep. 2024 Oct 10;14(1):23740. doi: 10.1038/s41598-024-74298-4. Sci Rep. 2024. PMID: 39390062 Free PMC article.
References
-
- Saigal S, Doyle LW. An overview of mortality and sequelae of preterm birth from infancy to adulthood. Lancet. 2008;371(9608):261–9. - PubMed
-
- Blencowe H, Cousens S, Oestergaard MZ, Chou D, Moller AB, Narwal R, Adler A, Vera Garcia C, Rohde S, Say L, et al. National, regional, and worldwide estimates of preterm birth rates in the year 2010 with time trends since 1990 for selected countries: a systematic analysis and implications. Lancet. 2012;379(9832):2162–72. - PubMed
-
- Larroque B, Marret S, Ancel PY, Arnaud C, Marpeau L, Supernant K, Pierrat V, Roze JC, Matis J, Cambonie G, et al. White matter damage and intraventricular hemorrhage in very preterm infants: the EPIPAGE study. J Pediatr. 2003;143(4):477–83. - PubMed
-
- Payne AH, Hintz SR, Hibbs AM, Walsh MC, Vohr BR, Bann CM, Wilson-Costello DE. Eunice Kennedy Shriver National Institute of child H, Human Development neonatal research N: neurodevelopmental outcomes of extremely low-gestational-age neonates with low-grade periventricular-intraventricular hemorrhage. JAMA Pediatr. 2013;167(5):451–9. - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
