

Application of opioid-free general anesthesia for gynecological laparoscopic surgery under ERAS protocol: a non-inferiority randomized controlled trial
- PMID: 36707777
- PMCID: PMC9881250
- DOI: 10.1186/s12871-023-01994-5
Application of opioid-free general anesthesia for gynecological laparoscopic surgery under ERAS protocol: a non-inferiority randomized controlled trial
Abstract
Background: Enhanced recovery after surgery (ERAS) is now widely used in various surgical fields including gynecological laparoscopic surgery, but the advantages of opioid-free anesthesia (OFA) in gynecological laparoscopic surgery under ERAS protocol are inexact.
Aims: This study aims to assess the effectiveness and feasibility of OFA technique versus traditional opioid-based anesthesia (OA) technique in gynecological laparoscopic surgery under ERAS.
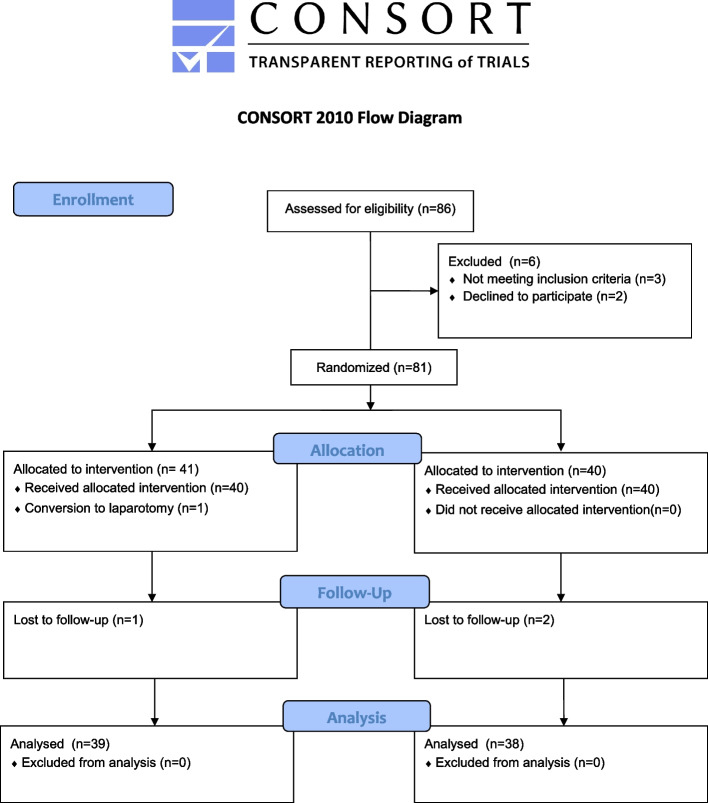
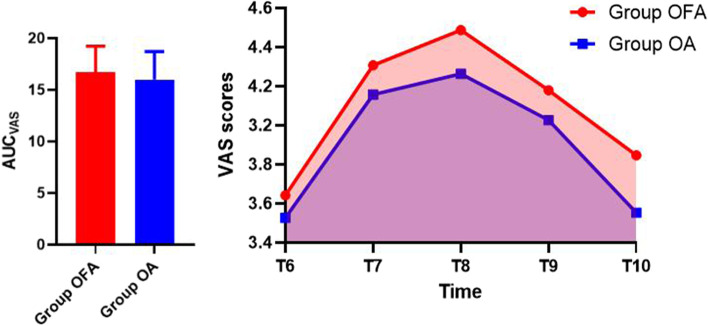
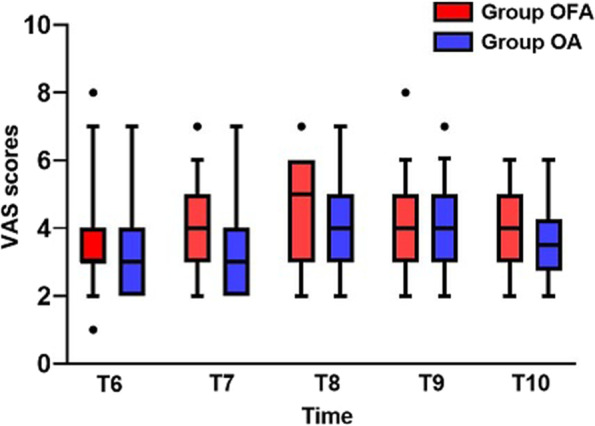
Methods: Adult female patients aged 18 ~ 65 years old undergoing gynecological laparoscopic surgery were randomly divided into OFA group (Group OFA, n = 39) with esketamine and dexmedetomidine or OA group (Group OA, n = 38) with sufentanil and remifentanil. All patients adopted ERAS protocol. The primary outcome was the area under the curve (AUC) of Visual Analogue Scale (VAS) scores (AUCVAS) postoperatively. Secondary outcomes included intraoperative hemodynamic variables, awakening and orientation recovery times, number of postoperative rescue analgesia required, incidence of postoperative nausea and vomiting (PONV) and Pittsburgh Sleep Quality Index (PSQI) perioperatively.
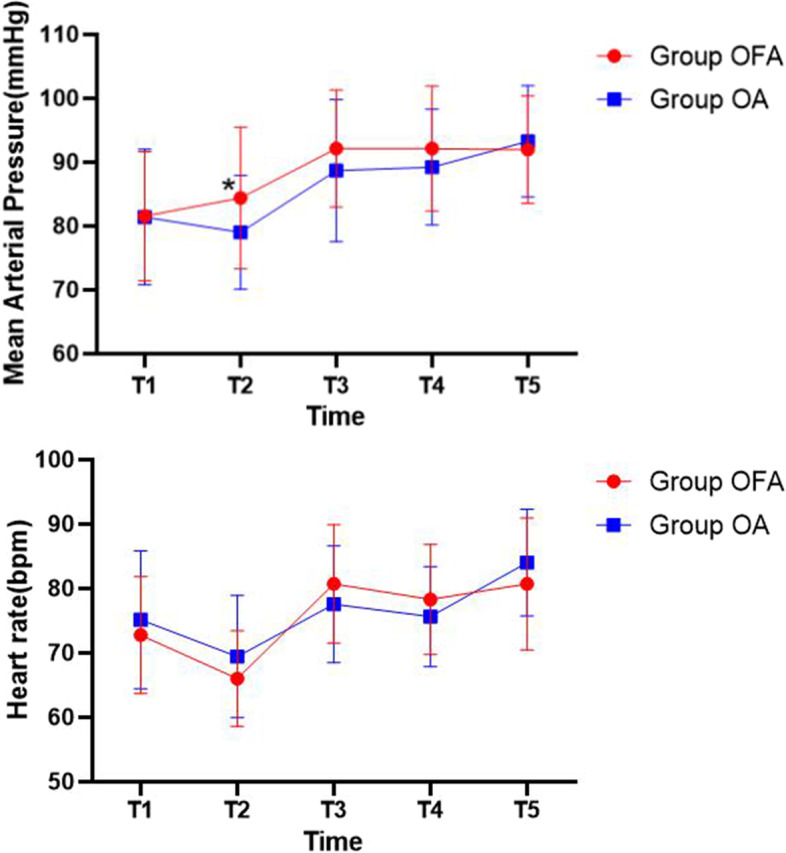
Results: AUCVAS was (Group OFA, 16.72 ± 2.50) vs (Group OA, 15.99 ± 2.72) (p = 0.223). No difference was found in the number of rescue analgesia required (p = 0.352). There were no between-group differences in mean arterial pressure (MAP) and heart rate (HR) (p = 0.211 and 0.659, respectively) except MAP at time of surgical incision immediately [(Group OFA, 84.38 ± 11.08) vs. (Group OA, 79.00 ± 8.92), p = 0.022]. Times of awakening and orientation recovery in group OFA (14.54 ± 4.22 and 20.69 ± 4.92, respectively) were both longer than which in group OA (12.63 ± 3.59 and 18.45 ± 4.08, respectively) (p = 0.036 and 0.033, respectively). The incidence of PONV in group OFA (10.1%) was lower than that in group OA (28.9%) significantly (p = 0.027). The postoperative PSQI was lower than the preoperative one in group OFA (p = 0.013).
Conclusion: In gynecological laparoscopic surgery under ERAS protocol, OFA technique is non-inferior to OA technique in analgesic effect and intraoperative anesthesia stability. Although awakening and orientation recovery times were prolonged compared to OA, OFA had lower incidence of PONV and improved postoperative sleep quality.
Trial registration: ChiCTR2100052761, 05/11/2021.
Keywords: Analgesia; ERAS; Gynecological Laparoscopic surgery; Non-inferiority; Opioid-free anesthesia.
© 2023. The Author(s).
Conflict of interest statement
We declare that we have no financial and personal relationships with other people or organizations that can inappropriately influence our work, there is no professional or other personal interest of any nature or kind in any product, service and/or company that could be construed as influencing the position presented in, or the review of, the manuscript entitled.
Figures
Similar articles
-
Safety and effectiveness of multimodal opioid-free anaesthesia for pain and recovery after laparoscopic surgery: a systematic review and meta-analysis.BMJ Open. 2025 Mar 22;15(3):e085988. doi: 10.1136/bmjopen-2024-085988. BMJ Open. 2025. PMID: 40122555 Free PMC article.
-
Opioid-free versus opioid-based anesthesia for day surgery laparoscopic inguinal hernia repair under ERAS protocol: a randomized non-inferiority trial.Hernia. 2025 Jul 9;29(1):225. doi: 10.1007/s10029-025-03410-y. Hernia. 2025. PMID: 40632161 Clinical Trial.
-
Opioid-free anesthesia with esketamine-dexmedetomidine versus opioid-based anesthesia with propofol-remifentanil in shoulder arthroscopy: a randomized controlled trial.BMC Surg. 2024 Aug 10;24(1):228. doi: 10.1186/s12893-024-02518-9. BMC Surg. 2024. PMID: 39127614 Free PMC article. Clinical Trial.
-
Opioid-free anesthesia improves postoperative recovery quality of small and medium-sized surgery: a prospective, randomized controlled study.Minerva Anestesiol. 2024 Sep;90(9):759-768. doi: 10.23736/S0375-9393.24.18125-4. Minerva Anestesiol. 2024. PMID: 39279482 Clinical Trial.
-
Opioid-Sparing Anesthesia Versus Opioid-Free Anesthesia for the Prevention of Postoperative Nausea and Vomiting after Laparoscopic Bariatric Surgery: A Systematic Review and Network Meta-Analysis.Anesth Analg. 2025 Feb 1;140(2):385-396. doi: 10.1213/ANE.0000000000006942. Epub 2024 Apr 5. Anesth Analg. 2025. PMID: 38578868
Cited by
-
Effect of comprehensive intervention model based on drug-psychology-society-skills on medication compliance and cognitive ability of chronic schizophrenia patients.World J Psychiatry. 2024 Dec 19;14(12):1947-1955. doi: 10.5498/wjp.v14.i12.1947. eCollection 2024 Dec 19. World J Psychiatry. 2024. PMID: 39704380 Free PMC article.
-
Safety and effectiveness of multimodal opioid-free anaesthesia for pain and recovery after laparoscopic surgery: a systematic review and meta-analysis.BMJ Open. 2025 Mar 22;15(3):e085988. doi: 10.1136/bmjopen-2024-085988. BMJ Open. 2025. PMID: 40122555 Free PMC article.
-
Respiratory training reduces postoperative pulmonary complications in elderly gynecological patients undergoing general anesthesia.Am J Transl Res. 2025 Jun 15;17(6):4612-4621. doi: 10.62347/VXSR1449. eCollection 2025. Am J Transl Res. 2025. PMID: 40672594 Free PMC article.
-
Rationale for the Use of Acupuncture to Stabilize Blood Pressure Fluctuations During Total Laparoscopic Hysterectomy: Protocol for a Pilot Parallel-Group Randomized Clinical Trial.JMIR Res Protoc. 2025 Jul 22;14:e77009. doi: 10.2196/77009. JMIR Res Protoc. 2025. PMID: 40603084 Free PMC article.
-
Opioid-Free Anesthesia for Pain Relief After Laparoscopic Cholecystectomy: A Prospective Randomized Controlled Trial.J Pain Res. 2023 Oct 30;16:3625-3632. doi: 10.2147/JPR.S432601. eCollection 2023. J Pain Res. 2023. PMID: 37928062 Free PMC article.
References
-
- Van den Beukel BA, de Ree R, van Leuven S, et al. Surgical treatment of adhesion-related chronic abdominal and pelvic pain after gynaecological and general surgery: a systematic review and meta-analysis. Hum Reprod Update. 2017;23(3):276–288. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
