

Limb loading enhances skill transfer between augmented and physical reality tasks during limb loss rehabilitation
- PMID: 36707817
- PMCID: PMC9881335
- DOI: 10.1186/s12984-023-01136-5
Limb loading enhances skill transfer between augmented and physical reality tasks during limb loss rehabilitation
Abstract
Background: Virtual and augmented reality (AR) have become popular modalities for training myoelectric prosthesis control with upper-limb amputees. While some systems have shown moderate success, it is unclear how well the complex motor skills learned in an AR simulation transfer to completing the same tasks in physical reality. Limb loading is a possible dimension of motor skill execution that is absent in current AR solutions that may help to increase skill transfer between the virtual and physical domains.
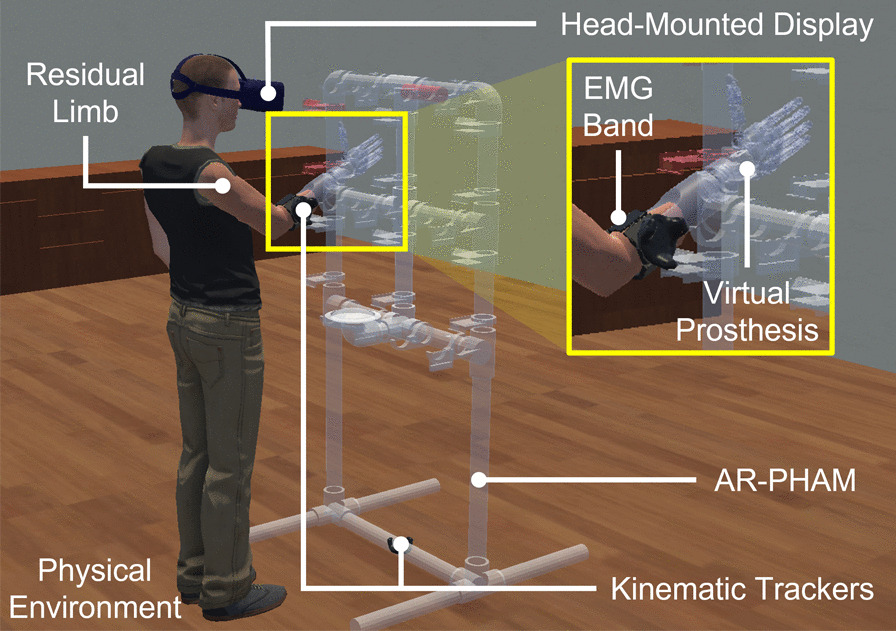
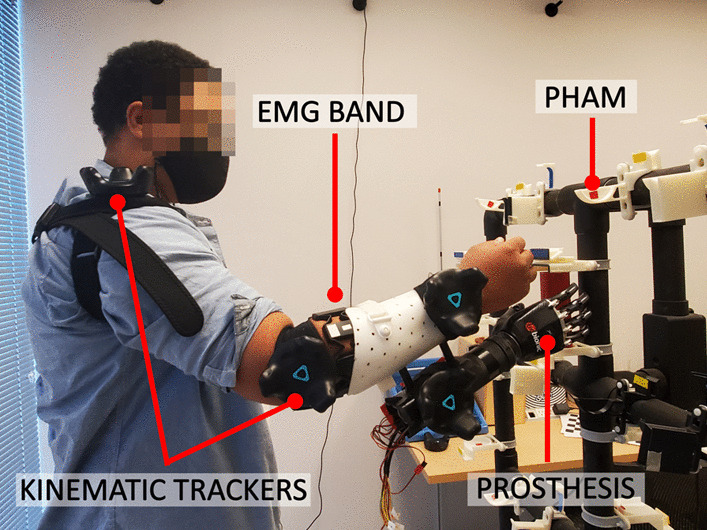
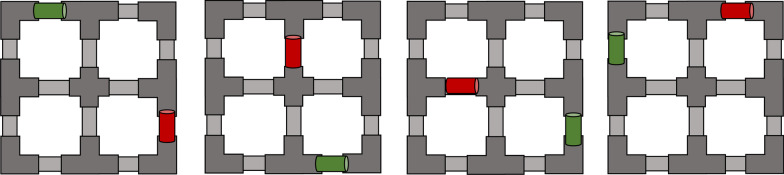
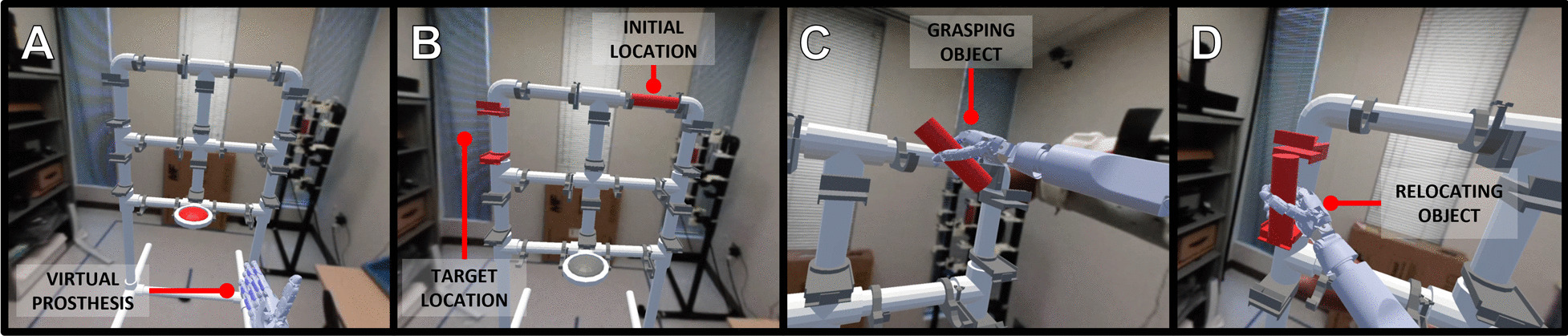
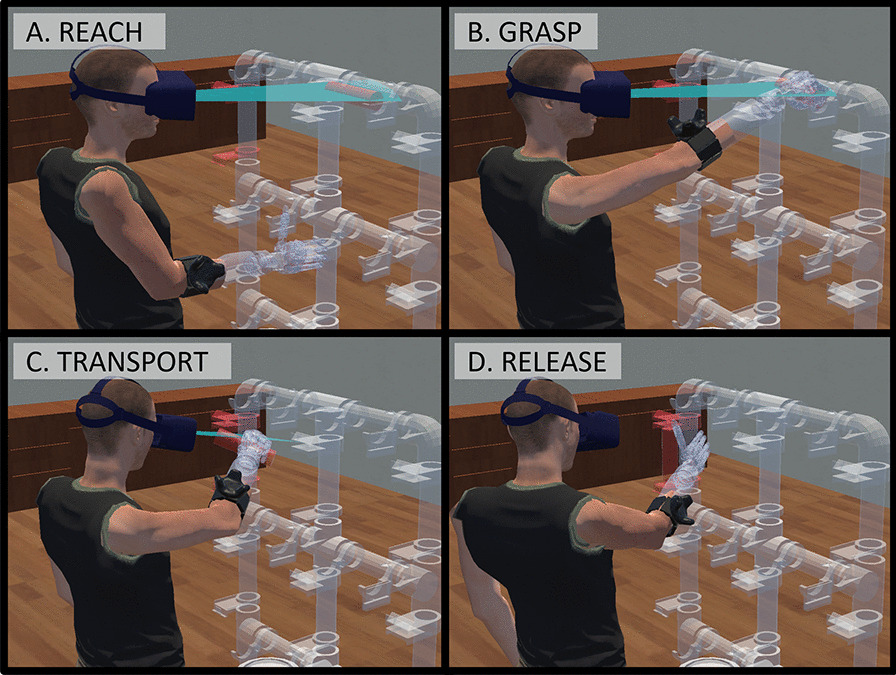
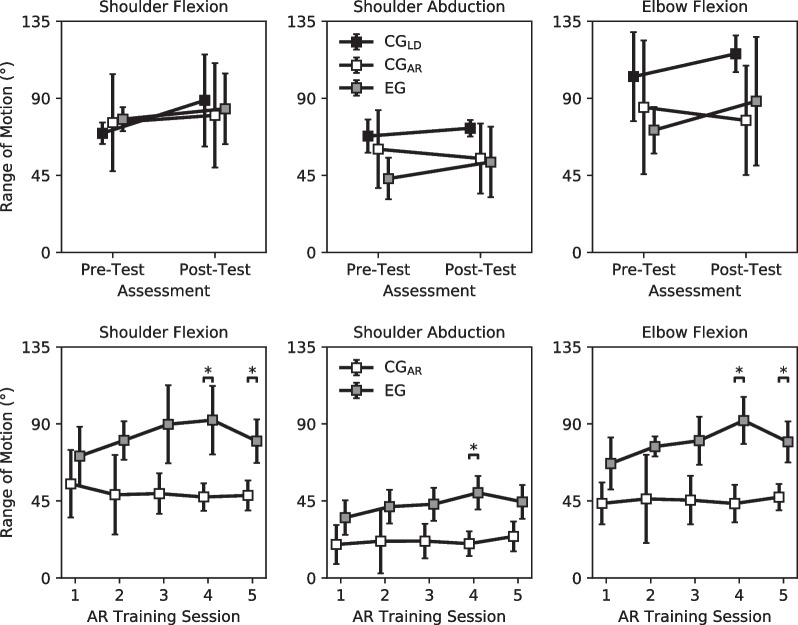
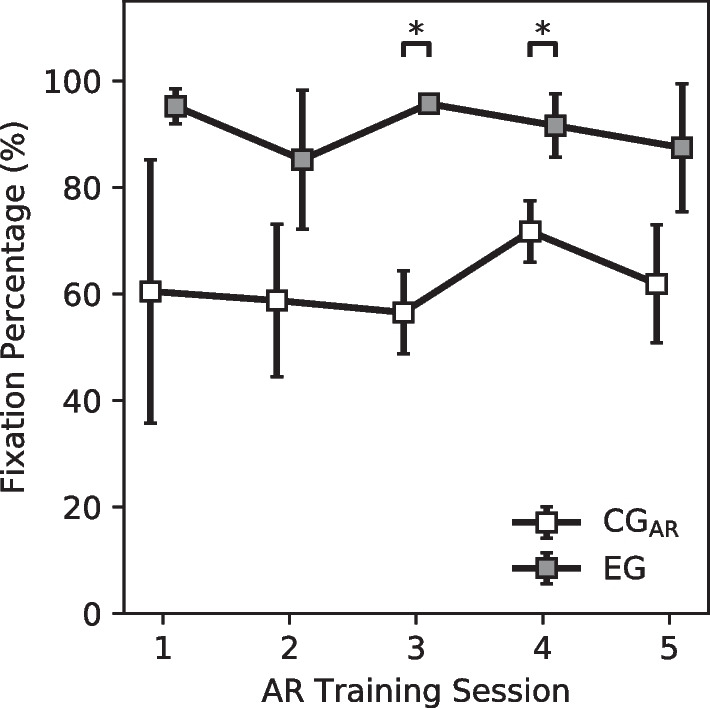
Methods: We implemented an immersive AR environment where individuals could operate a myoelectric virtual prosthesis to accomplish a variety of object relocation manipulations. Intact limb participants were separated into three groups, the load control (CGLD; [Formula: see text]), the AR control (CGAR; [Formula: see text]), and the experimental group (EG; [Formula: see text]). Both the CGAR and EG completed a 5-session prosthesis training protocol in AR while the CGLD performed simple muscle training. The EG attempted manipulations in AR while undergoing limb loading. The CGAR attempted the same manipulations without loading. All participants performed the same manipulations in physical reality while operating a real prosthesis pre- and post-training. The main outcome measure was the change in the number of manipulations completed during the physical reality assessments (i.e. completion rate). Secondary outcomes included movement kinematics and visuomotor behavior.
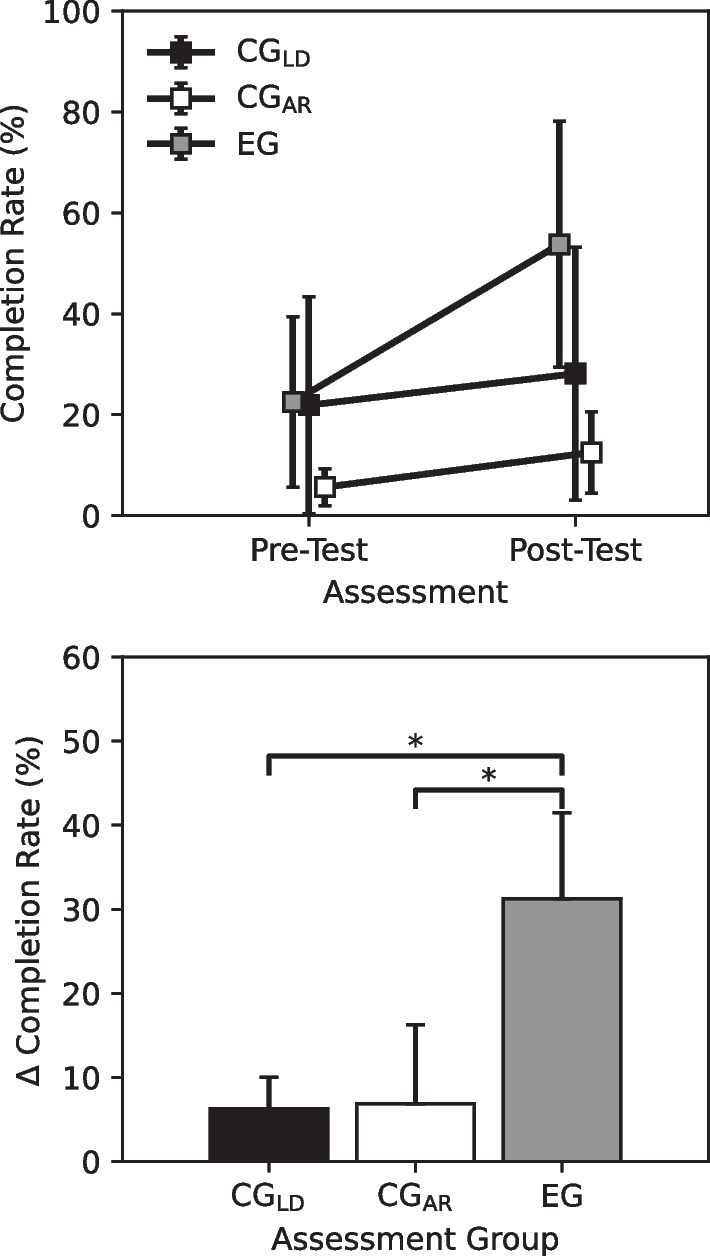
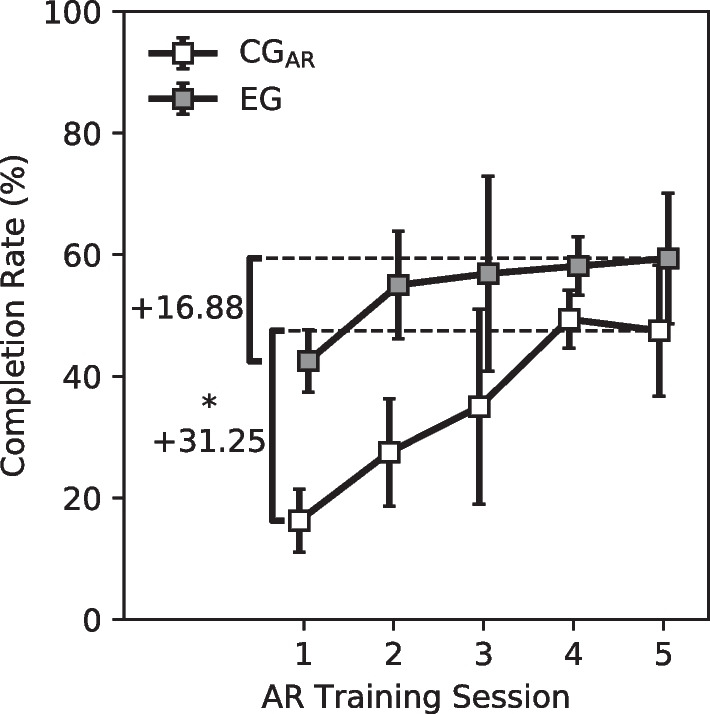
Results: The EG experienced a greater increase in completion rate post-training than both the CGAR and CGLD. This performance increase was accompanied by a shorter motor learning phase, the EG's performance saturating in less sessions of AR training than the CGAR.
Conclusion: The results demonstrated that limb loading plays an important role in transferring complex motor skills learned in virtual spaces to their physical reality analogs. While participants who did not receive limb loading were able to receive some functional benefit from AR training, participants who received the loading experienced a greater positive change in motor performance with their performance saturating in fewer training sessions.
Keywords: Augmented reality; Myoelectric control; Proprioception; Upper-limb prostheses.
© 2023. The Author(s).
Conflict of interest statement
Dr. Thakor has an ownership interest in Infinite Biomedical Technologies, a prosthesis technology company. Dr. Kaliki is employed by Infinite Biomedical Technologies. Competing interest are managed by the Johns Hopkins University Conflict Review Committee.
Figures
References
-
- Resnik L, Borgia M, Cancio J, Heckman J, Highsmith J, Levy C, Phillips S, Webster J. Dexterity, activity performance, disability, quality of life, and independence in upper limb veteran prosthesis users: a normative study. Disabil Rehabil. 2020;44:1–12. - PubMed
-
- Staff N. Amputation statistics by cause, limb loss in the united states. Knoxville: National Limb Loss Information Center; 2008.
-
- Ziegler-Graham K, MacKenzie EJ, Ephraim PL, Travison TG, Brookmeyer R. Estimating the prevalence of limb loss in the United States: 2005 to 2050. Arch Phys Med Rehabil. 2008;89(3):422–429. - PubMed
-
- Parker PA, Scott RN. Myoelectric control of prostheses. Crit Rev Biomed Eng. 1986;13(4):283–310. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
