

Internet-delivered cognitive behavioural therapy for insomnia disorder in depressed patients treated at an outpatient clinic for mood disorders: protocol of a randomised controlled trial
- PMID: 36707843
- PMCID: PMC9880372
- DOI: 10.1186/s12888-022-04492-z
Internet-delivered cognitive behavioural therapy for insomnia disorder in depressed patients treated at an outpatient clinic for mood disorders: protocol of a randomised controlled trial
Abstract
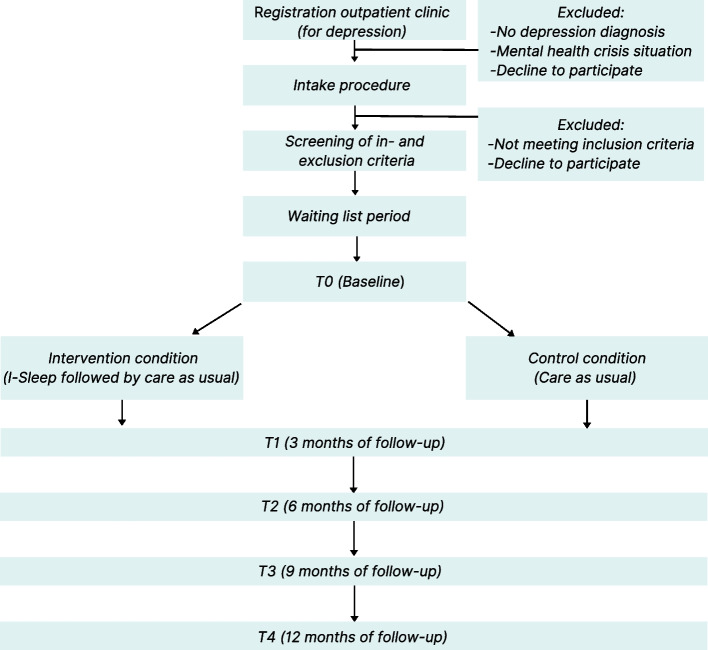
Background: Major depression is a highly prevalent disorder causing severe personal distress, and high societal costs. Patients with depression often have comorbid insomnia disorder (ID) leading to even worse personal distress and worse treatment outcomes. Recent results from a non-randomised pilot study with internet-delivered Cognitive Behavioural Therapy (CBTi) for Insomnia (I-Sleep) added to regular depression care were promising regarding feasibility and initial effects on insomnia complaints and depression. However, no randomised controlled trial (RCT) has been performed yet to access the (cost-) effectiveness of I-Sleep for depression. Therefore, this protocol article presents the design of an RCT aimed to assess the (cost-) effectiveness of I-Sleep in addition to usual care for depression compared to usual care alone in depressed patients with a comorbid Insomnia Disorder (ID) treated at outpatient clinics for mood disorders. METHODS /DESIGN: This is a multi-centre RCT with measurements at baseline and at 3, 6, 9, and 12 months of follow-up. Patients with depression and an ID are randomised to either I-Sleep treatment followed by regular depression care or to regular depression care alone. Our aim is to recruit one hundred and seventy-five patients from multiple outpatient clinics for mood disorders. The primary outcome is the change in depressive symptoms over 12 months of follow-up measured with the Patient Health Questionnaire (PHQ-9). Secondary outcomes are recovery from depression (PHQ-9), insomnia severity (Insomnia Severity Index, ISI), daily functioning (Work and Social Adjustment Scale, WSAS), general quality of life (EuroQol 5-level version, EQ-5D-5L), and societal costs (Adapted versions of the iMTA Productivity Cost Questionnaire, iPCQ and iMTA Medical Cost Questionnaire, iMCQ).
Discussion: We hypothesize that the addition of I-Sleep to usual care will result in a significant improvement in depression treatment outcomes and quality of life as well as a decrease in healthcare and societal costs compared to usual care alone. This study is the first pragmatic RCT evaluating the effectiveness and cost-effectiveness of adding CBTi to usual care for depression.
Trial registration: Netherlands Trial Register (NL8955). Registered on October 6th2020. https://trialsearch.who.int/Trial2.aspx?TrialID=NL8955.
Keywords: Cognitive behavioural therapy for insomnia (CBTi); Cost-effectiveness; Depression; I-Sleep; Insomnia disorder (ID); Internet-delivered; Randomised controlled trial (RCT); e-health.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Cost-effectiveness of i-Sleep, a guided online CBT intervention, for patients with insomnia in general practice: protocol of a pragmatic randomized controlled trial.BMC Psychiatry. 2016 Apr 2;16:85. doi: 10.1186/s12888-016-0783-z. BMC Psychiatry. 2016. PMID: 27038786 Free PMC article. Clinical Trial.
-
Group cognitive behavioural therapy for insomnia compared with treatment as usual for sleep problems in psychiatric care (the SIP trials): a protocol for a pragmatic, randomised controlled trial.BMJ Open. 2025 Apr 17;15(4):e090997. doi: 10.1136/bmjopen-2024-090997. BMJ Open. 2025. PMID: 40250874 Free PMC article.
-
Randomised controlled trial on the effect of internet-delivered computerised cognitive-behavioural therapy on patients with insomnia who remain symptomatic following hypnotics: a study protocol.BMJ Open. 2018 Jan 30;8(1):e018220. doi: 10.1136/bmjopen-2017-018220. BMJ Open. 2018. PMID: 29382675 Free PMC article. Clinical Trial.
-
Internet-Delivered Cognitive Behavioral Therapy for Insomnia: Tailoring Cognitive Behavioral Therapy for Insomnia for Patients with Chronic Insomnia.Sleep Med Clin. 2020 Jun;15(2):117-131. doi: 10.1016/j.jsmc.2020.02.001. Sleep Med Clin. 2020. PMID: 32386688 Review.
-
Internet-Delivered Cognitive Behavioral Therapy for Insomnia: Tailoring Cognitive Behavioral Therapy for Insomnia for Patients with Chronic Insomnia.Sleep Med Clin. 2019 Sep;14(3):301-315. doi: 10.1016/j.jsmc.2019.04.002. Epub 2019 Jun 5. Sleep Med Clin. 2019. PMID: 31375200 Review.
Cited by
-
A Pilot Nurse-Administered CBT Intervention for Insomnia in Patients with Schizophrenic Disorder: A Randomized Clinical Effectiveness Trial.J Clin Med. 2023 Sep 23;12(19):6147. doi: 10.3390/jcm12196147. J Clin Med. 2023. PMID: 37834794 Free PMC article.
-
Applying therapist-guided digital cognitive behavioral therapy for insomnia in psychiatry: a mixed-methods process evaluation.BMC Psychiatry. 2025 Apr 28;25(1):428. doi: 10.1186/s12888-025-06824-1. BMC Psychiatry. 2025. PMID: 40296081 Free PMC article.
-
Exploring the Causal Relationship Between Migraine and Insomnia Through Bidirectional Two-Sample Mendelian Randomization: A Bidirectional Causal Relationship.J Pain Res. 2024 Jul 16;17:2407-2415. doi: 10.2147/JPR.S460566. eCollection 2024. J Pain Res. 2024. PMID: 39050680 Free PMC article.
-
Metabolic Characteristics of Gut Microbiota and Insomnia: Evidence from a Mendelian Randomization Analysis.Nutrients. 2024 Sep 2;16(17):2943. doi: 10.3390/nu16172943. Nutrients. 2024. PMID: 39275260 Free PMC article.
References
-
- James SL, Abate D, Abate KH, Abay SM, Abbafati C, Abbasi N, et al. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018;392(10159):1789–858. [cited 2023 Jan 17]. Available from: https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(18)32279.... - PMC - PubMed
-
- Ten Have M, Penninx BWJH, Tuithof M, van Dorsselaer S, Kleinjan M, Spijker J, et al. Duration of major and minor depressive episodes and associated risk indicators in a psychiatric epidemiological cohort study of the general population. Acta Psychiatr Scand. 2017;136(3):300–12. doi: 10.1111/acps.12753. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
