

Toward nutrition improving outcome of critically ill patients: How to interpret recent feeding RCTs?
- PMID: 36707883
- PMCID: PMC9883882
- DOI: 10.1186/s13054-023-04317-9
Toward nutrition improving outcome of critically ill patients: How to interpret recent feeding RCTs?
Abstract
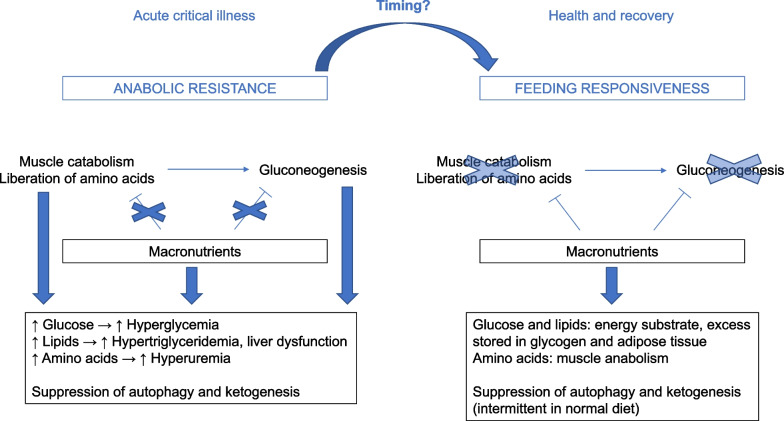
Although numerous observational studies associated underfeeding with poor outcome, recent randomized controlled trials (RCTs) have shown that early full nutritional support does not benefit critically ill patients and may induce dose-dependent harm. Some researchers have suggested that the absence of benefit in RCTs may be attributed to overrepresentation of patients deemed at low nutritional risk, or to a too low amino acid versus non-protein energy dose in the nutritional formula. However, these hypotheses have not been confirmed by strong evidence. RCTs have not revealed any subgroup benefiting from early full nutritional support, nor benefit from increased amino acid doses or from indirect calorimetry-based energy dosing targeted at 100% of energy expenditure. Mechanistic studies attributed the absence of benefit of early feeding to anabolic resistance and futile catabolism of extra provided amino acids, and to feeding-induced suppression of recovery-enhancing pathways such as autophagy and ketogenesis, which opened perspectives for fasting-mimicking diets and ketone supplementation. Yet, the presence or absence of an anabolic response to feeding cannot be predicted or monitored and likely differs over time and among patients. In the absence of such monitor, the value of indirect calorimetry seems obscure, especially in the acute phase of illness. Until now, large feeding RCTs have focused on interventions that were initiated in the first week of critical illness. There are no large RCTs that investigated the impact of different feeding strategies initiated after the acute phase and continued after discharge from the intensive care unit in patients recovering from critical illness.
Keywords: Amino acid; Autophagy; Critical illness; Energy target; Enteral nutrition; Indirect calorimetry; Intermittent feeding; Ketone; Parenteral nutrition.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Hermans G, Van Mechelen H, Clerckx B, Vanhullebusch T, Mesotten D, Wilmer A, et al. Acute outcomes and 1-year mortality of intensive care unit-acquired weakness: a cohort study and propensity-matched analysis. Am J Respir Crit Care Med. 2014;190(4):410–420. - PubMed
-
- Herridge MS, Tansey CM, Matte A, Tomlinson G, Diaz-Granados N, Cooper A, et al. Functional disability 5 years after acute respiratory distress syndrome. N Engl J Med. 2011;364(14):1293–1304. - PubMed
-
- Van Aerde N, Meersseman P, Debaveye Y, Wilmer A, Gunst J, Casaer MP, et al. Five-year impact of ICU-acquired neuromuscular complications: a prospective, observational study. Intensive Care Med. 2020;46(6):1184–1193. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
