

Combination of external fixation using digital six-axis fixator and internal fixation to treat severe complex knee deformity
- PMID: 36707900
- PMCID: PMC9881260
- DOI: 10.1186/s13018-023-03530-0
Combination of external fixation using digital six-axis fixator and internal fixation to treat severe complex knee deformity
Abstract
Background: Severe knee valgus/varus or complex multiplanar deformities are common in clinic. If not corrected in time, cartilage wear will be aggravated and initiate the osteoarthritis due to lower limb malalignment. Internal fixation is unable to correct severe complex deformities, especially when combined with lower limb discrepancy (LLD). Based on the self-designed digital six-axis external fixator Q spatial fixator (QSF), which can correct complex multiplanar deformities without changing structures, accuracy of correction can be improved significantly.
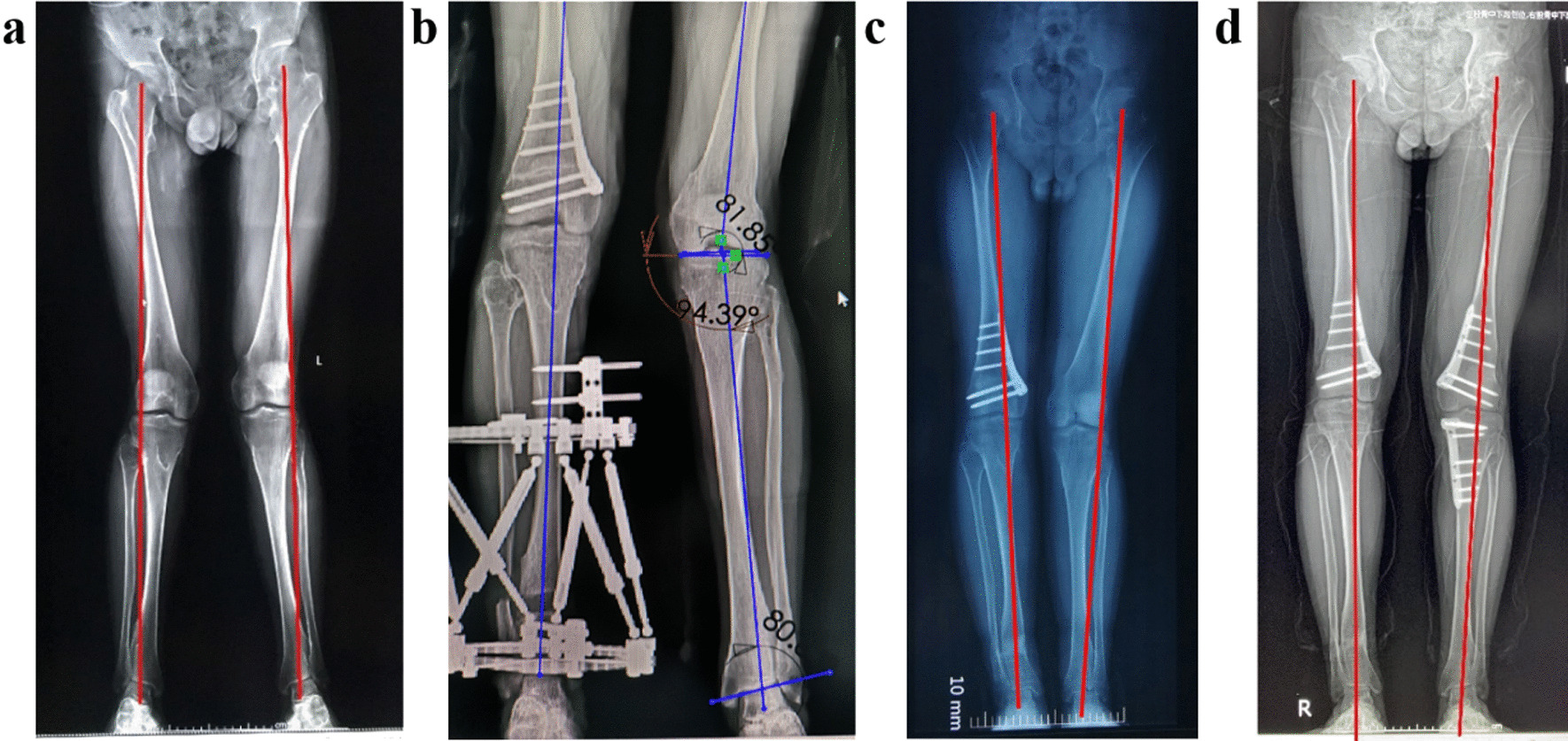
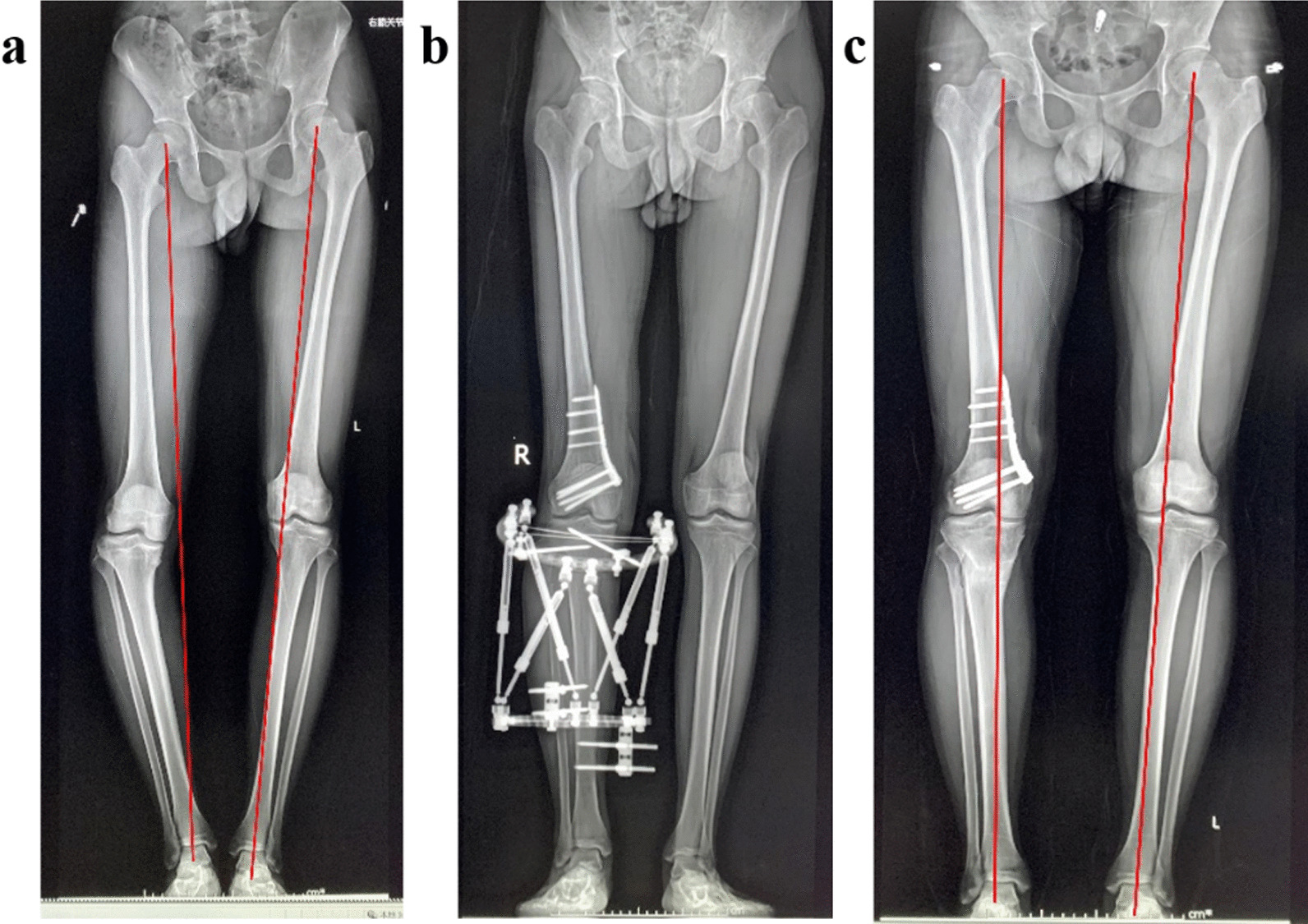
Methods: This retrospective study included 24 patients who suffered from complex knee deformity with LLD treated by QSF and internal fixation at our institution from January 2018 to February 2021. All patients had a closing wedge distal femoral osteotomy with internal fixation for immediate correction and high tibia osteotomy with QSF fixation for postoperative progressive correction. Data of correction prescriptions were computed by software from postoperative CT scans.
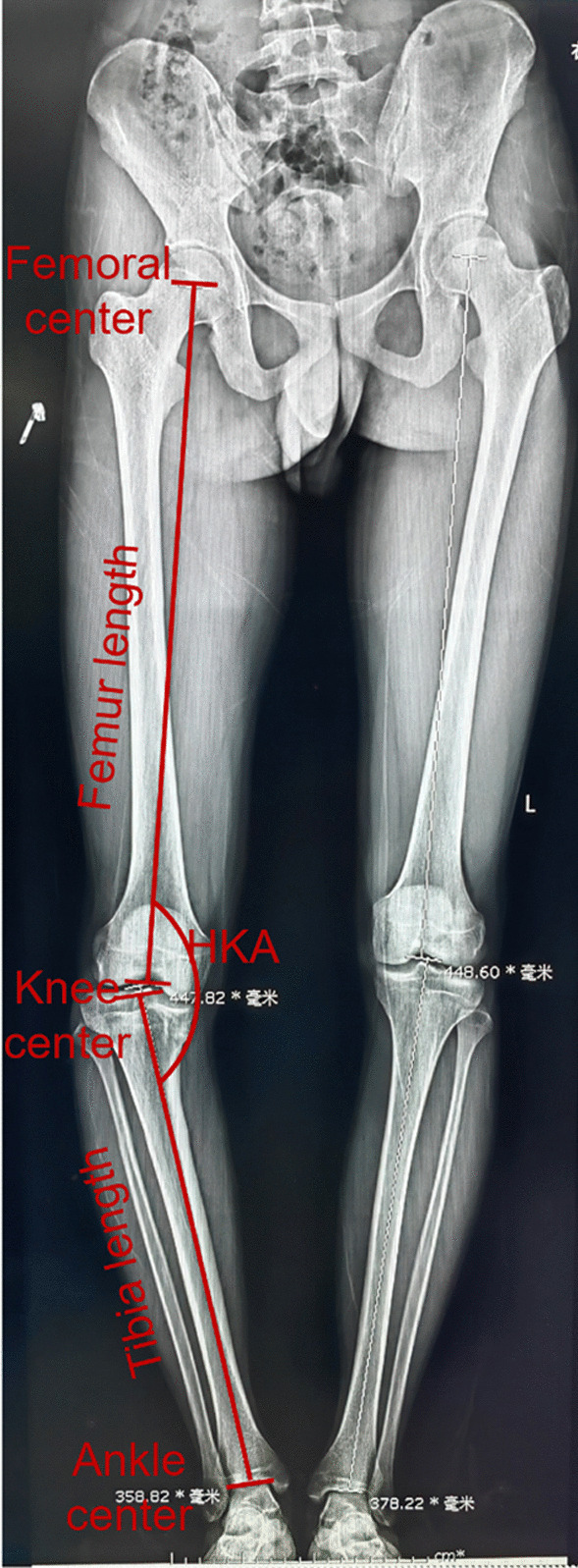
Results: Mean discrepancy length of operative side was 2.39 ± 1.04 cm (range 0.9-4.4 cm) preoperatively. The mean difference of lower limb was 0.32 ± 0.13 cm (range 0.11-0.58 cm) postoperatively. The length of limb correction had significant difference (p < 0.05). The mean MAD and HKA decreased significantly (p < 0.05), and the mean MPTA and LDFA increased significantly (p < 0.05). There were significant increase (p < 0.05) in the AKSS-O, AKSS-F and Tegner Activity Score. The lower limb alignment was corrected (p < 0.05). The mean time of removing external fixator was 112.8 ± 17.9 days (range 83-147 days).
Conclusions: Complex knee deformity with LLD can be treated by six-axis external fixator with internal fixation without total knee arthroplasty. Lower limb malalignment and discrepancy can be corrected precisely and effectively by this approach.
Keywords: Knee; Osteotomy; Q spatial fixator (QSF); Valgus; Varus.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

Similar articles
-
[Correction of tibial multiplanar deformities using single Taylor external fixator combined with biplanar osteotomy].Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2023 Jul 15;37(7):839-845. doi: 10.7507/1002-1892.202303121. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2023. PMID: 37460181 Free PMC article. Chinese.
-
Evaluation of the external fixator TrueLok Hexapod System for tibial deformity correction in children.Orthop Traumatol Surg Res. 2017 Sep;103(5):761-764. doi: 10.1016/j.otsr.2017.03.015. Epub 2017 Apr 17. Orthop Traumatol Surg Res. 2017. PMID: 28428035
-
Correction of severe lower extremity deformity with digital hexapod external fixator based on CT data.Eur J Med Res. 2022 Nov 17;27(1):252. doi: 10.1186/s40001-022-00887-6. Eur J Med Res. 2022. PMID: 36397115 Free PMC article.
-
[Corrective osteotomies around the knee joint using hexapods].Oper Orthop Traumatol. 2024 Apr;36(2):83-95. doi: 10.1007/s00064-023-00836-4. Epub 2023 Nov 10. Oper Orthop Traumatol. 2024. PMID: 37947855 Review. German.
-
[Osteotomies for deformity correction on the pediatric knee].Unfallchirurg. 2019 Jan;122(1):33-43. doi: 10.1007/s00113-018-0593-5. Unfallchirurg. 2019. PMID: 30607483 Review. German.
Cited by
-
In vivo axial load-share ratio measurement using a novel hexapod system for safe external fixator removal.BMC Musculoskelet Disord. 2024 May 9;25(1):353. doi: 10.1186/s12891-024-07440-y. BMC Musculoskelet Disord. 2024. PMID: 38724941 Free PMC article.
-
Measurement of the dynamic axial load-share ratio in vivo could indicate sufficient callus healing in external fixators.BMC Musculoskelet Disord. 2025 Feb 12;26(1):139. doi: 10.1186/s12891-025-08353-0. BMC Musculoskelet Disord. 2025. PMID: 39940030 Free PMC article.
-
Digitized Precision Corrective Osteotomy for Treating Knee Joint Deformities: Current Evidence and Future Perspectives.Orthop Surg. 2025 Aug;17(8):2221-2233. doi: 10.1111/os.70085. Epub 2025 May 29. Orthop Surg. 2025. PMID: 40441744 Free PMC article. Review.
References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
