

An Interventional Response Phenotyping Study in Chronic Low Back Pain: Protocol for a Mechanistic Randomized Controlled Trial
- PMID: 36708026
- PMCID: PMC10403311
- DOI: 10.1093/pm/pnad005
An Interventional Response Phenotyping Study in Chronic Low Back Pain: Protocol for a Mechanistic Randomized Controlled Trial
Abstract
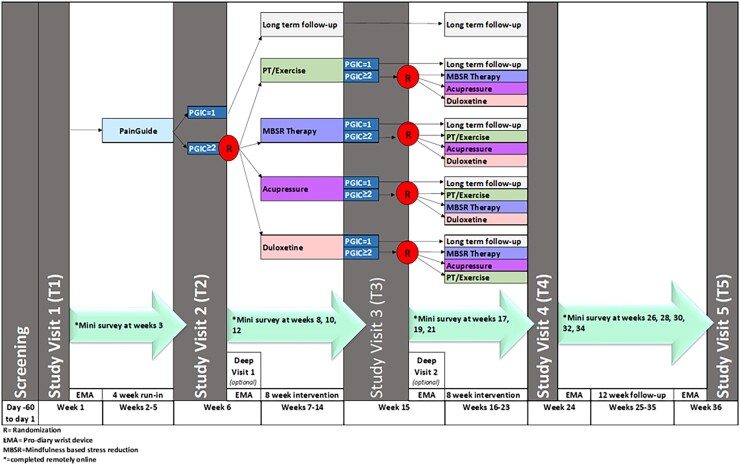
Evidence-based treatments for chronic low back pain (cLBP) typically work well in only a fraction of patients, and at present there is little guidance regarding what treatment should be used in which patients. Our central hypothesis is that an interventional response phenotyping study can identify individuals with different underlying mechanisms for their pain who thus respond differentially to evidence-based treatments for cLBP. Thus, we will conduct a randomized controlled Sequential, Multiple Assessment, Randomized Trial (SMART) design study in cLBP with the following three aims. Aim 1: Perform an interventional response phenotyping study in a cohort of cLBP patients (n = 400), who will receive a sequence of interventions known to be effective in cLBP. For 4 weeks, all cLBP participants will receive a web-based pain self-management program as part of a run-in period, then individuals who report no or minimal improvement will be randomized to: a) mindfulness-based stress reduction, b) physical therapy and exercise, c) acupressure self-management, and d) duloxetine. After 8 weeks, individuals who remain symptomatic will be re-randomized to a different treatment for an additional 8 weeks. Using those data, we will identify the subsets of participants that respond to each treatment. In Aim 2, we will show that currently available, clinically derived measures, can predict differential responsiveness to the treatments. In Aim 3, a subset of participants will receive deeper phenotyping (n = 160), to identify new experimental measures that predict differential responsiveness to the treatments, as well as to infer mechanisms of action. Deep phenotyping will include functional neuroimaging, quantitative sensory testing, measures of inflammation, and measures of autonomic tone.
© The Author(s) 2023. Published by Oxford University Press on behalf of the American Academy of Pain Medicine.
Figures
Similar articles
-
A prospective randomized controlled study of auricular point acupressure to manage chronic low back pain in older adults: study protocol.Trials. 2020 Jan 20;21(1):99. doi: 10.1186/s13063-019-4016-x. Trials. 2020. PMID: 31959226 Free PMC article.
-
The RESOLVE Trial for people with chronic low back pain: protocol for a randomised clinical trial.J Physiother. 2017 Jan;63(1):47-48. doi: 10.1016/j.jphys.2016.11.001. Epub 2016 Nov 14. J Physiother. 2017. PMID: 27939089
-
Effectiveness, costs and cost-effectiveness of chiropractic care and physiotherapy compared with information and advice in the treatment of non-specific chronic low back pain: study protocol for a randomised controlled trial.Trials. 2017 Dec 22;18(1):613. doi: 10.1186/s13063-017-2351-3. Trials. 2017. PMID: 29273083 Free PMC article.
-
Meditation-Based Therapy for Chronic Low Back Pain Management: A Systematic Review and Meta-Analysis of Randomized Controlled Trials.Pain Med. 2022 Sep 30;23(10):1800-1811. doi: 10.1093/pm/pnac037. Pain Med. 2022. PMID: 35226059
-
Yoga compared to non-exercise or physical therapy exercise on pain, disability, and quality of life for patients with chronic low back pain: A systematic review and meta-analysis of randomized controlled trials.PLoS One. 2020 Sep 1;15(9):e0238544. doi: 10.1371/journal.pone.0238544. eCollection 2020. PLoS One. 2020. PMID: 32870936 Free PMC article.
Cited by
-
Towards precision medicine in clinical trials for the treatment of urologic chronic pelvic pain syndrome: lessons from the MAPP Research Network.Nat Rev Urol. 2025 Apr 30. doi: 10.1038/s41585-025-01030-w. Online ahead of print. Nat Rev Urol. 2025. PMID: 40307537 Review.
-
Design characteristics of Sequential Multiple Assignment Randomized Trials (SMARTs) for human health: a scoping review of studies between 2009-2024.medRxiv [Preprint]. 2025 Jun 8:2025.06.06.25329149. doi: 10.1101/2025.06.06.25329149. medRxiv. 2025. PMID: 40502556 Free PMC article. Preprint.
-
The use of sequential multiple assignment randomized trials (SMARTs) in physical activity interventions: a systematic review.BMC Med Res Methodol. 2024 Dec 19;24(1):308. doi: 10.1186/s12874-024-02439-4. BMC Med Res Methodol. 2024. PMID: 39701990 Free PMC article.
-
A randomized controlled trial of graded exposure treatment (GET living) for adolescents with chronic pain.Pain. 2024 Jan 1;165(1):177-191. doi: 10.1097/j.pain.0000000000003010. Epub 2023 Aug 25. Pain. 2024. PMID: 37624900 Free PMC article. Clinical Trial.
-
Baseline predictors of responders to auricular point acupressure in chronic low back pain.Clin Tradit Med Pharmacol. 2025 Jun;6(2):200215. doi: 10.1016/j.ctmp.2025.200215. Epub 2025 Apr 14. Clin Tradit Med Pharmacol. 2025. PMID: 40417635 Free PMC article.
References
-
- Manchikanti L, Singh V, Falco FJ, Benyamin RM, Hirsch JA.. Epidemiology of low back pain in adults. Neuromodulation. 2014;17(Suppl 2):3–10. - PubMed
-
- Clauw DJ. Fibromyalgia: a clinical review. JAMA. 2014;311(15):1547–1555. - PubMed
-
- Nuesch E, Hauser W, Bernardy K, Barth J, Juni P.. Comparative efficacy of pharmacological and non-pharmacological interventions in fibromyalgia syndrome: network meta-analysis. Ann Rheum Dis. 2013;72(6):955–962. - PubMed
-
- Abdel Shaheed C, Maher CG, Williams KA, Day R, McLachlan AJ.. Efficacy, tolerability, and dose-dependent effects of opioid analgesics for low back pain: a systematic review and meta-analysis. JAMA Intern Med. 2016;176(7):958. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
