

Point-of-care fluorescence imaging reveals extent of bacterial load in diabetic foot ulcers
- PMID: 36708275
- PMCID: PMC9885466
- DOI: 10.1111/iwj.14080
Point-of-care fluorescence imaging reveals extent of bacterial load in diabetic foot ulcers
Abstract
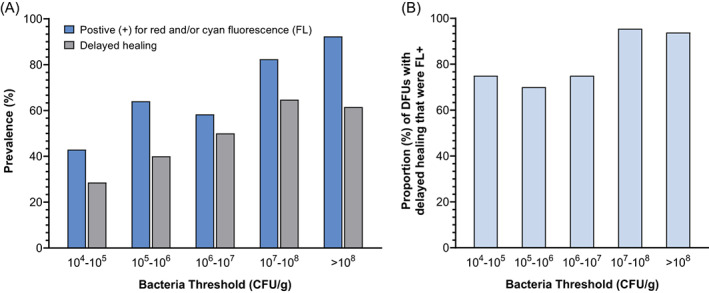
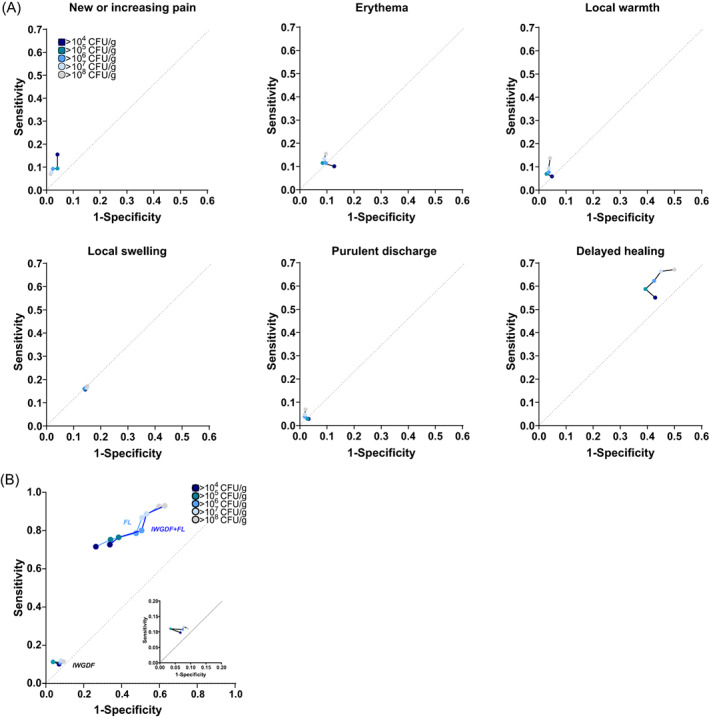
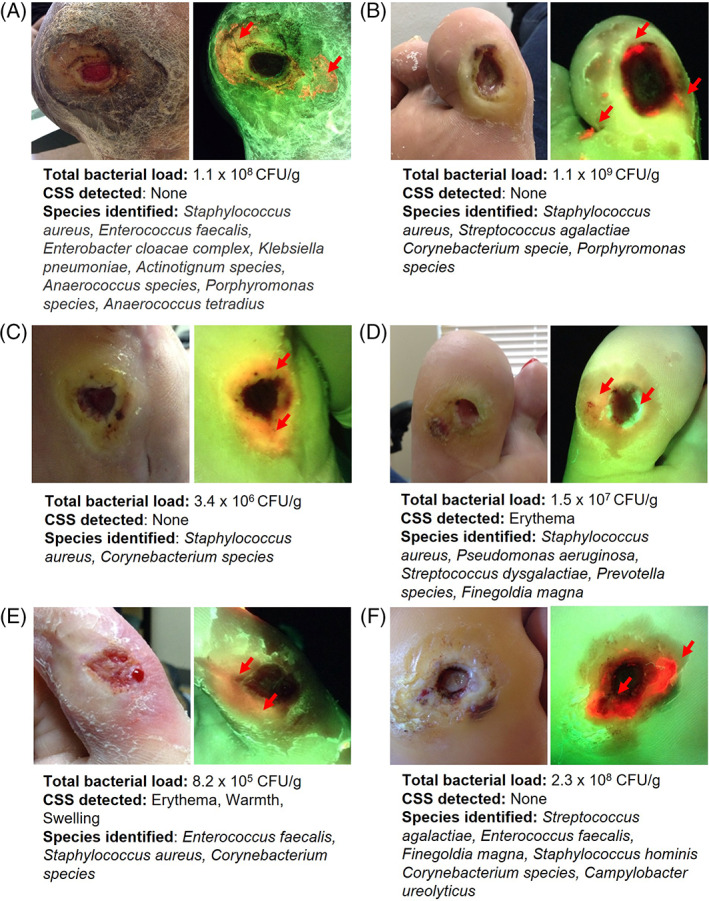
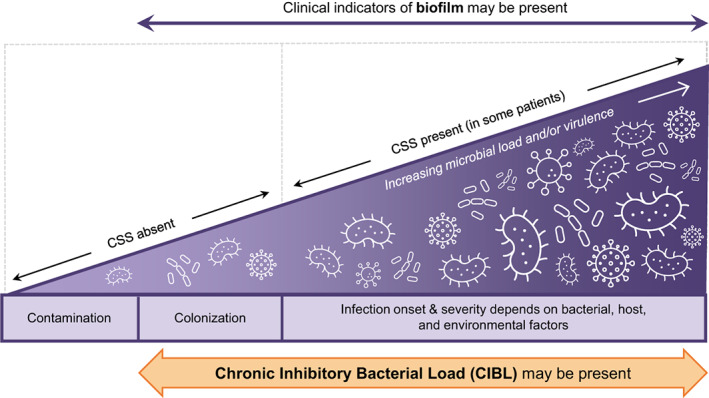
Elevated levels of bacteria, including biofilm, increase the risk of chronic wound infection and inhibit healing. Addressing asymptomatic high bacterial loads is challenged by a lack of clinical terminology and diagnostic tools. This post-hoc multicenter clinical trial analysis of 138 diabetic foot ulcers investigates fluorescence (FL)-imaging role in detecting biofilm-encased and planktonic bacteria in wounds at high loads. The sensitivity and specificity of clinical assessment and FL-imaging were compared across bacterial loads of concern (104 -109 CFU/g). Quantitative tissue culture confirmed the total loads. Bacterial presence was confirmed in 131/138 ulcers. Of these, 93.9% had loads >104 CFU/g. In those wounds, symptoms of infection were largely absent and did not correlate with, or increase proportionately with, bacterial loads at any threshold. FL-imaging increased sensitivity for the detection of bacteria across loads 104 -109 (P < .0001), peaking at 92.6% for >108 CFU/g. Imaging further showed that 84.2% of ulcers contained high loads in the periwound region. New terminology, chronic inhibitory bacterial load (CIBL), describes frequently asymptomatic, high bacterial loads in diabetic ulcers and periwound tissues, which require clinical intervention to prevent sequelae of infection. We anticipate this will spark a paradigm shift in assessment and management, enabling earlier intervention along the bacterial-infection continuum and supporting improved wound outcomes.
Keywords: bacterial load; diabetic foot; fluorescence imaging; infection; wound healing.
© 2023 The Authors. International Wound Journal published by Medicalhelplines.com Inc (3M) and John Wiley & Sons Ltd.
Conflict of interest statement
TES received funding from MolecuLight Inc., to cover conduct of the study. No competing financial interest exists for other authors.
Figures
Similar articles
-
Diagnostic Accuracy of Point-of-Care Fluorescence Imaging for the Detection of Bacterial Burden in Wounds: Results from the 350-Patient Fluorescence Imaging Assessment and Guidance Trial.Adv Wound Care (New Rochelle). 2021 Mar;10(3):123-136. doi: 10.1089/wound.2020.1272. Epub 2020 Sep 25. Adv Wound Care (New Rochelle). 2021. PMID: 32870774 Free PMC article.
-
Real-time bacterial fluorescence imaging accurately identifies wounds with moderate-to-heavy bacterial burden.J Wound Care. 2019 Jun 2;28(6):346-357. doi: 10.12968/jowc.2019.28.6.346. J Wound Care. 2019. PMID: 31166857
-
Improving Wound Healing and Infection Control in Long-term Care with Bacterial Fluorescence Imaging.Adv Skin Wound Care. 2024 Sep 1;37(9):471-479. doi: 10.1097/ASW.0000000000000177. Epub 2024 Jul 17. Adv Skin Wound Care. 2024. PMID: 39023985
-
Systematic reviews of wound care management: (3) antimicrobial agents for chronic wounds; (4) diabetic foot ulceration.Health Technol Assess. 2000;4(21):1-237. Health Technol Assess. 2000. PMID: 11074391 Review.
-
The pH of wound fluid in diabetic foot ulcers -- the way forward in detecting clinical infection?Curr Diabetes Rev. 2014 May;10(3):177-81. doi: 10.2174/1573399810666140609143217. Curr Diabetes Rev. 2014. PMID: 24912533 Review.
Cited by
-
Determination of the Course of Cyan Fluorescence of Pseudomonas aeruginosa with a Handheld Bacterial Imaging Device.Diagnostics (Basel). 2024 Jul 10;14(14):1474. doi: 10.3390/diagnostics14141474. Diagnostics (Basel). 2024. PMID: 39061611 Free PMC article.
-
Integration of Functional Polymers and Biosensors to Enhance Wound Healing.Adv Healthc Mater. 2024 Nov;13(29):e2401461. doi: 10.1002/adhm.202401461. Epub 2024 Sep 5. Adv Healthc Mater. 2024. PMID: 39235365 Free PMC article. Review.
-
Pressure injuries and biofilms: Microbiome, model systems and therapies.Wound Repair Regen. 2025 Jan-Feb;33(1):e70005. doi: 10.1111/wrr.70005. Wound Repair Regen. 2025. PMID: 39949184 Free PMC article. Review.
-
From prototype to implementation: Development of the DMIST scoring system for monitoring diabetic foot ulcers.GHM Open. 2025 Jun 30;5(1):52-57. doi: 10.35772/ghmo.2023.01024. GHM Open. 2025. PMID: 40621123 Free PMC article.
-
Point-of-care fluorescence imaging to optimise wound bed preparation prior to cellular and/or tissue-based product (CTP) application.Int Wound J. 2023 Nov;20(9):3441-3442. doi: 10.1111/iwj.14446. Epub 2023 Oct 17. Int Wound J. 2023. PMID: 37846207 Free PMC article. No abstract available.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
