

Expecting more: the case for incorporating fertility services into comprehensive sickle cell disease care
- PMID: 36708736
- PMCID: PMC10318482
- DOI: 10.1016/S2352-3026(22)00353-2
Expecting more: the case for incorporating fertility services into comprehensive sickle cell disease care
Abstract
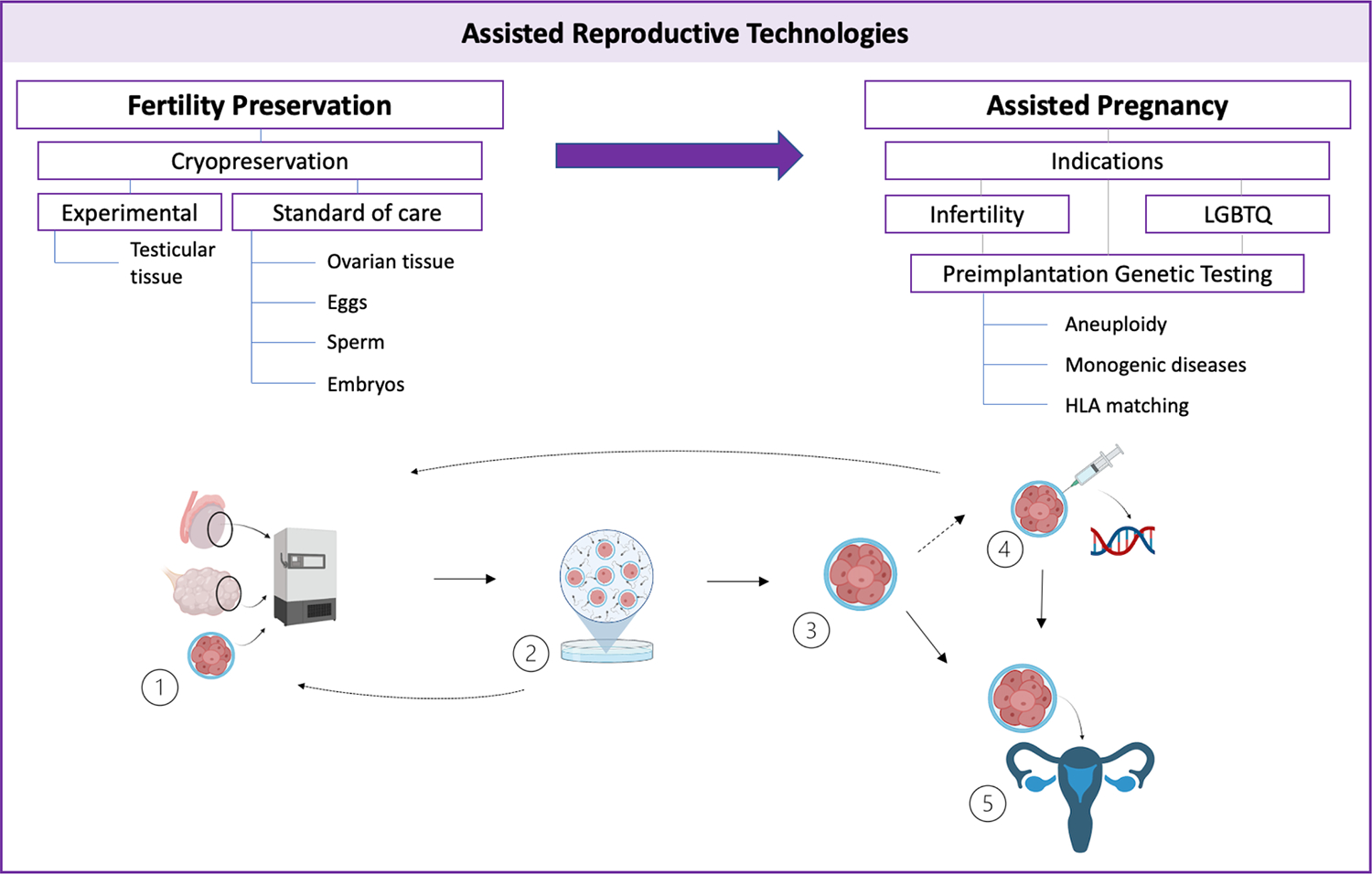
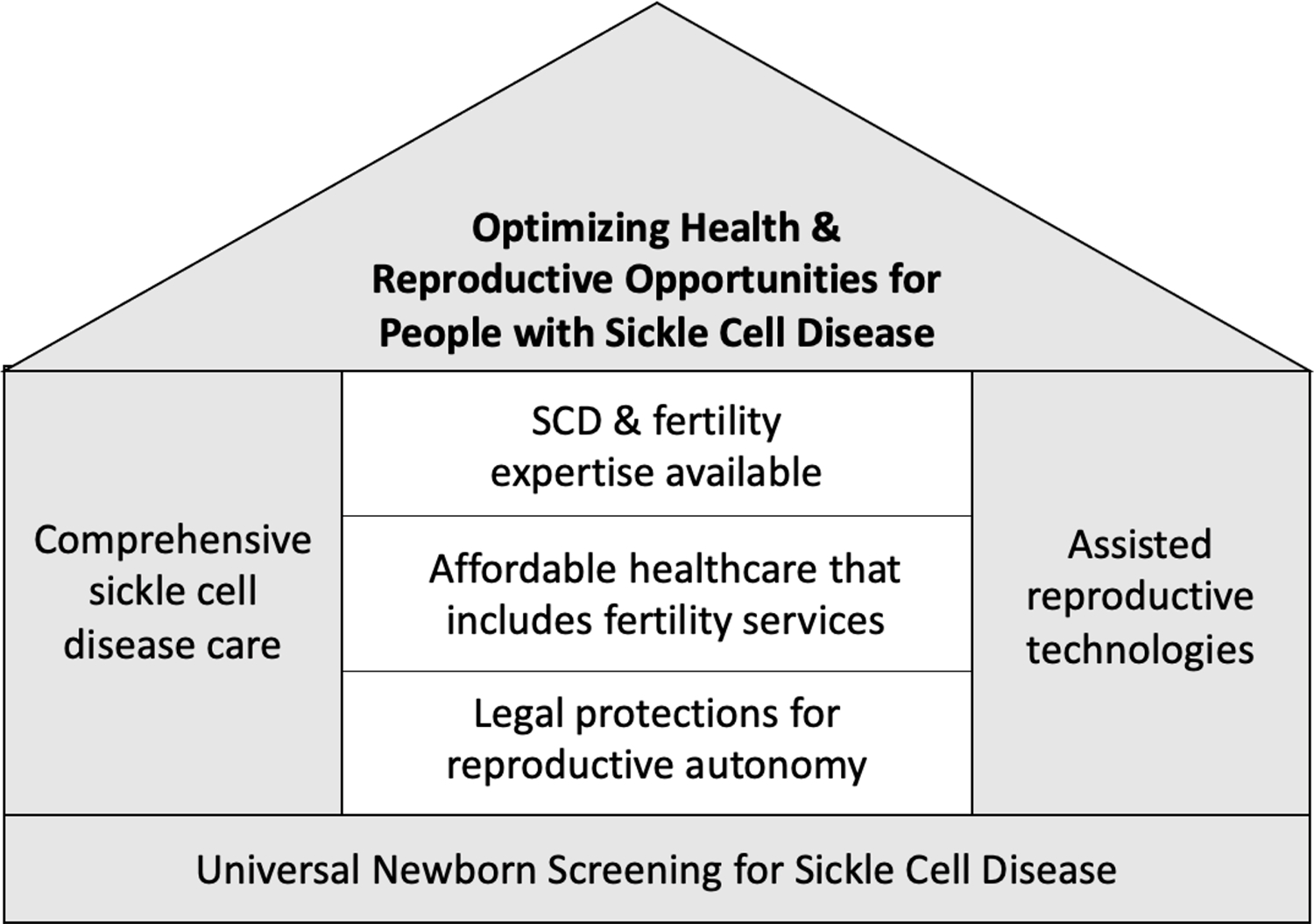
Assisted reproductive technologies (ART) are not yet systematically available to people with sickle cell disease or their parents. Fertility care for these groups requires addressing sickle cell disease-associated infertility risks, fertility preservation options, pregnancy possibilities and outcomes, and, when needed, infertility treatment. People with a chance of having a child with sickle cell disease can use in-vitro fertilisation with preimplantation genetic testing to conceive a child unaffected by sickle cell disease. Also, parents of children with sickle cell disease can use this technology to identify embryos to become potential future matched sibling donors for stem cell transplant. In the USA, disparities in fertility care for the sickle cell disease community are especially stark. Universal screening of newborn babies' identifies sickle cell disease and sickle cell trait, guidelines direct preconception genetic carrier screening, and standard-of-care fertility preserving options exist. However, potentially transformative treatments and cures for patients with sickle cell disease are not used due to iatrogenic infertility concerns. In diversely resourced care settings, obstacles to providing fertility care to people affected by sickle cell disease persist. In this Viewpoint, we contend that fertility care should be incorporated into the comprehensive care model for sickle cell disease, supporting alignment of treatment goals with reproductive life plans and delivering on the promise of individualised high-quality care for people with sickle cell disease and their families. We consider the obligation to provide fertility care in light of medical evidence, with acknowledgment of formidable obstacles to optimising care, and powerful historical and ethical considerations.
Copyright © 2023 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Declaration of interests LHP declares grant funding from National Institutes of Health (NIH)/National Heart, Lung, and Blood Institute K23HL146841 and U01 HL156620-01, the American Society of Hematology, Doris Duke Charitable Foundation Grant number 2020147, and the Mellon Foundation; consulting fees from Global Blood Therapeutics and Novo Nordisk; support for meeting attendance from the American Society of Hematology and the Hemostasis and Thrombosis Research Society; serves on the CRESCENT data safety monitoring board and is an advisor to the Sickle Cell Reproductive Health Education Directive; and serves in a leadership role at the Foundation for Women and Girls with Blood Disorders' Sickle Cell Disease Learning Action Network and on the American Society of Hematology's Maternal Health Working Group. AN declares grant funding from Global Blood Therapeutics; consulting fees from Global Blood Therapeutics, Bluebird Bio, Novartis, and Dispersol; received honoraria from the American Society of Pediatric Hematology; support for meeting attendance from the Foundation for Women and Girls with Blood Disorders; serves on data safety monitoring boards for Editas Medicine, the PIVOT Trial and the PUSH UP Trail; and serves in a leadership role at the Foundation for Women and Girls with Blood Disorders' Sickle Cell Disease Learning Action Network. SL declares grant funding from Patient-Centered Outcomes Research Institute (PCORI), Health Resources and Services Administration (HRSA), Maryland Community Health Resources Commission (CHRC MD) National Institutes of Health (NIH); consulting fees from Novartis, Pfizer, Bluebird Bio, Novo Nordisk, and Magenta; participates in data safety monitoring boards for Observational Study Monitoring Board, Sickle Pan-African Research Consortium (NIH) and on an ad hoc basis for American Society for Blood and Marrow Transplantation; serves the Vice President of the National Alliance for Sickle Cell Centers; and holds stock in Pfzier and Teva Pharmaceuticals. TW declares consulting fees from Agios Pharmaceuticals, Novo Nordisk, Fulcrum, Global Blood Therapeutics, and Bluebird Bio and support for travel provided by Agios Pharmaceuticals. ADM declares honoraria from PhenX, and support from the Arthur Wharton Foundation. All other authors have no competing interests.
Figures
Similar articles
-
Sickle cell disease and infertility risks: implications for counseling and care of affected girls and women.Expert Rev Hematol. 2024 Aug;17(8):493-504. doi: 10.1080/17474086.2024.2372320. Epub 2024 Jun 26. Expert Rev Hematol. 2024. PMID: 38913857 Free PMC article. Review.
-
No crystal stair: supporting fertility care and the pursuit of pregnancy in women with sickle cell disease.Hematology Am Soc Hematol Educ Program. 2022 Dec 9;2022(1):459-466. doi: 10.1182/hematology.2022000381. Hematology Am Soc Hematol Educ Program. 2022. PMID: 36485154 Free PMC article.
-
Fertility challenges for women with sickle cell disease.Expert Rev Hematol. 2017 Oct;10(10):891-901. doi: 10.1080/17474086.2017.1367279. Epub 2017 Sep 11. Expert Rev Hematol. 2017. PMID: 28891355 Review.
-
Pregnancy outcomes after assisted human reproduction.J Obstet Gynaecol Can. 2014 Jan;36(1):64-83. doi: 10.1016/S1701-2163(15)30685-X. J Obstet Gynaecol Can. 2014. PMID: 24444289
-
Reproductive intentions in mothers of young children with sickle cell disease.Pediatr Blood Cancer. 2020 May;67(5):e28227. doi: 10.1002/pbc.28227. Epub 2020 Feb 17. Pediatr Blood Cancer. 2020. PMID: 32065500
Cited by
-
Access to assisted reproductive technologies in sub-Saharan Africa: fertility professionals' views.Sex Reprod Health Matters. 2024 Dec;32(1):2355790. doi: 10.1080/26410397.2024.2355790. Epub 2024 Jun 12. Sex Reprod Health Matters. 2024. PMID: 38864373 Free PMC article.
-
Using the consolidated framework for implementation research to identify challenges and opportunities for implementing a reproductive health education program into sickle cell disease care.J Pediatr Psychol. 2025 Jan 1;50(1):30-39. doi: 10.1093/jpepsy/jsae031. J Pediatr Psychol. 2025. PMID: 38699955 Free PMC article.
-
Insights Into the Expectations of Infertile Men Regarding Multidisciplinary Reproductive Health Services.Health Expect. 2025 Aug;28(4):e70327. doi: 10.1111/hex.70327. Health Expect. 2025. PMID: 40590245 Free PMC article.
-
Addressing fertility in adolescent boys with sickle cell disease: emerging clinical and ethical dilemmas.Blood Adv. 2023 Sep 26;7(18):5351-5353. doi: 10.1182/bloodadvances.2023010292. Blood Adv. 2023. PMID: 37155994 Free PMC article. No abstract available.
-
Infertility and treatment-seeking practices among females and males with sickle cell disease in the Sickle Cell Disease Implementation Consortium registry.Pediatr Blood Cancer. 2023 Jul;70(7):e30356. doi: 10.1002/pbc.30356. Epub 2023 Apr 14. Pediatr Blood Cancer. 2023. PMID: 37057750 Free PMC article.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
