

Genomic characterisation of hormone receptor-positive breast cancer arising in very young women
- PMID: 36709040
- PMCID: PMC10619213
- DOI: 10.1016/j.annonc.2023.01.009
Genomic characterisation of hormone receptor-positive breast cancer arising in very young women
Abstract
Background: Very young premenopausal women diagnosed with hormone receptor-positive, human epidermal growth factor receptor 2-negative (HR+HER2-) early breast cancer (EBC) have higher rates of recurrence and death for reasons that remain largely unexplained.
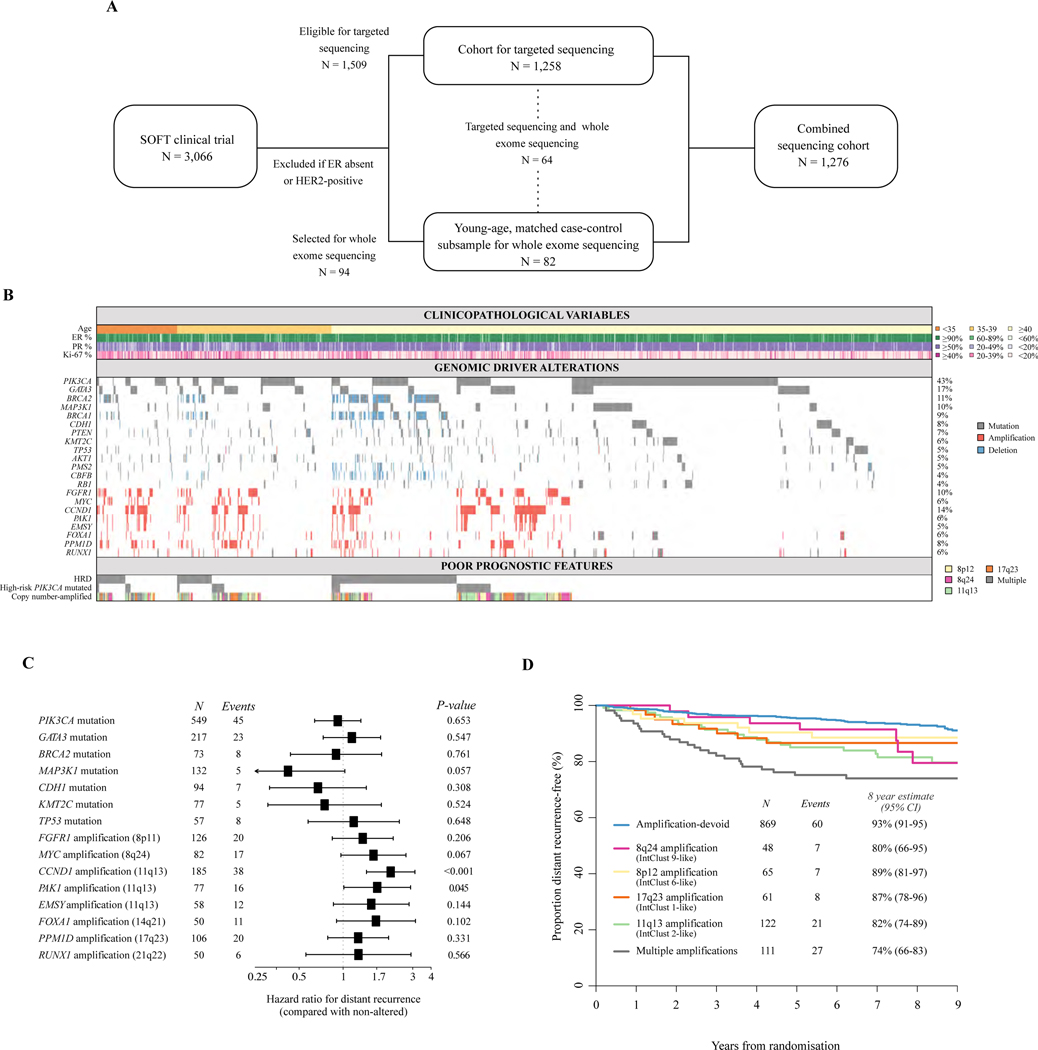
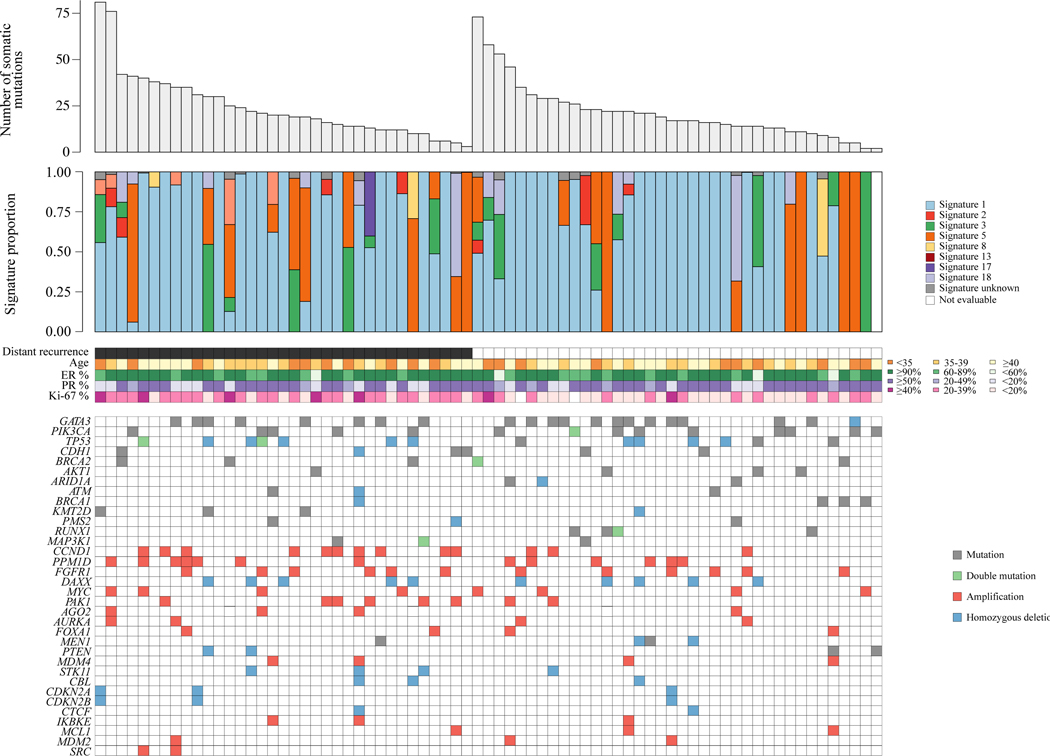
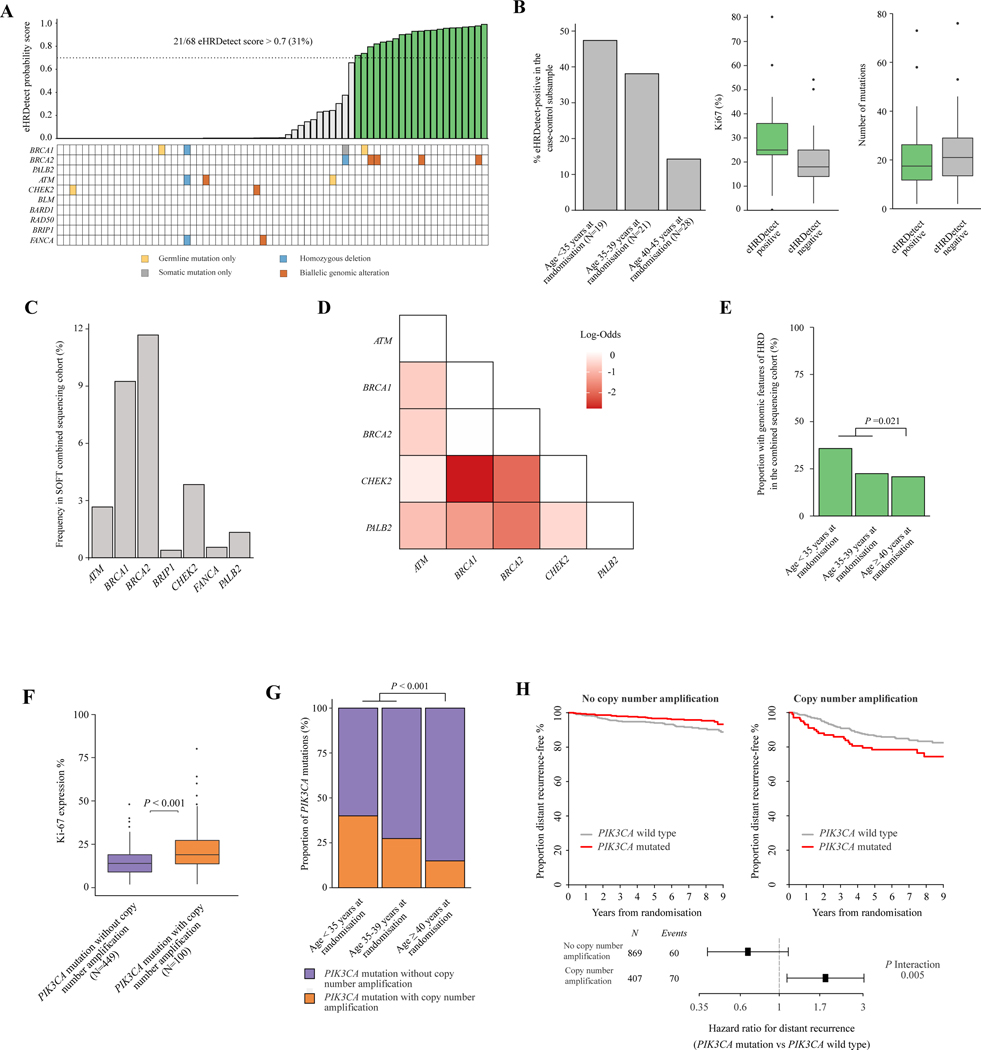
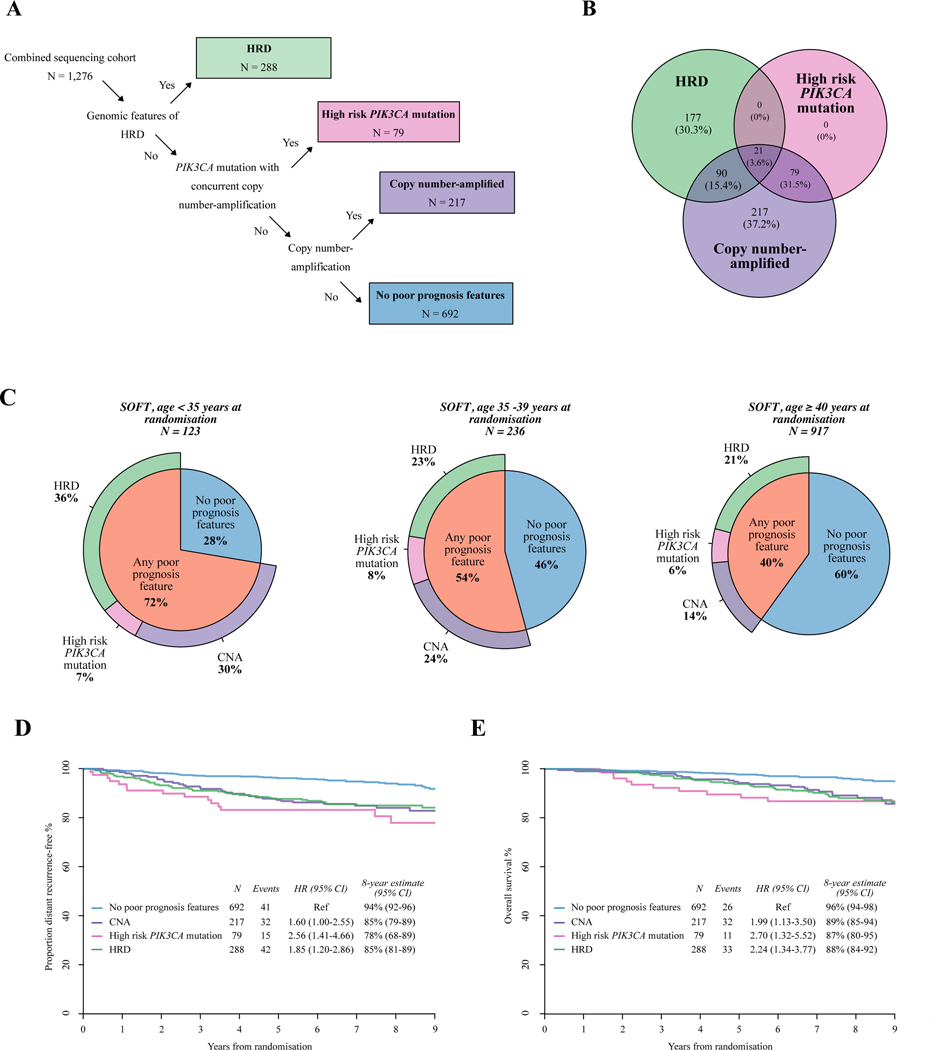
Patients and methods: Genomic sequencing was applied to HR+HER2- tumours from patients enrolled in the Suppression of Ovarian Function Trial (SOFT) to determine genomic drivers that are enriched in young premenopausal women. Genomic alterations were characterised using next-generation sequencing from a subset of 1276 patients (deep targeted sequencing, n = 1258; whole-exome sequencing in a young-age, case-control subsample, n = 82). We defined copy number (CN) subgroups and assessed for features suggestive of homologous recombination deficiency (HRD). Genomic alteration frequencies were compared between young premenopausal women (<40 years) and older premenopausal women (≥40 years), and assessed for associations with distant recurrence-free interval (DRFI) and overall survival (OS).
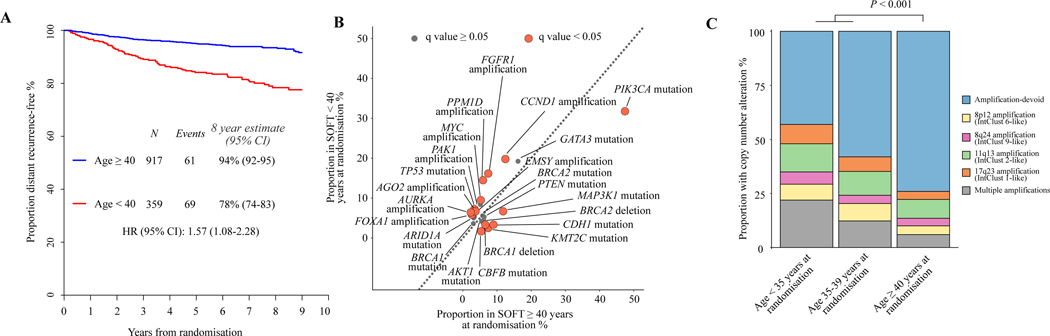
Results: Younger women (<40 years, n = 359) compared with older women (≥40 years, n = 917) had significantly higher frequencies of mutations in GATA3 (19% versus 16%) and CN amplifications (CNAs) (47% versus 26%), but significantly lower frequencies of mutations in PIK3CA (32% versus 47%), CDH1 (3% versus 9%), and MAP3K1 (7% versus 12%). Additionally, they had significantly higher frequencies of features suggestive of HRD (27% versus 21%) and a higher proportion of PIK3CA mutations with concurrent CNAs (23% versus 11%). Genomic features suggestive of HRD, PIK3CA mutations with CNAs, and CNAs were associated with significantly worse DRFI and OS compared with those without these features. These poor prognostic features were enriched in younger patients: present in 72% of patients aged <35 years, 54% aged 35-39 years, and 40% aged ≥40 years. Poor prognostic features [n = 584 (46%)] versus none [n = 692 (54%)] had an 8-year DRFI of 84% versus 94% and OS of 88% versus 96%. Younger women (<40 years) had the poorest outcomes: 8-year DRFI 74% versus 85% and OS 80% versus 93%, respectively.
Conclusion: These results provide insights into genomic alterations that are enriched in young women with HR+HER2- EBC, provide rationale for genomic subgrouping, and highlight priority molecular targets for future clinical trials.
Keywords: breast cancer; genomics; hormone receptor positive; prognosis; young women.
Copyright © 2023 European Society for Medical Oncology. Published by Elsevier Ltd. All rights reserved.
Conflict of interest statement
Disclosure GV has received honoraria (outside of this submitted study) from MSD Oncology, Roche, Pfizer, Novartis, Bayer, Daiichi Sankyo, and Dako Agilent. SNZ declares multiple patents on mutational signature-based algorithms including HRDetect. PS has acted as an uncompensated consultant for Roche-Genentech. EC declares consulting or advisory role for Lilly, Novartis, MSD, AstraZeneca, Pfizer, Roche; speakers’ bureau for Lilly, Roche, Pfizer; travel accommodation and expenses from Pfizer and Roche. PK has research contracts with PFS genomics and Prelude DX. MCl declares honoraria from BMS, Astellas, Janssen, MSD, Sanofi, Bayer, Roche, Pfizer, Novartis, Ipsen; consultation for BMS, MSD, Bayer, EUNSA, Pfizer, Roche, Janssen, Pierre Fabre, Ipsen; travel funding from Janssen, Astellas, Roche, Ipsen, MSD. CG declares travel expenses from Genentech, Roche, Daiichi-Sankyo, AstraZeneca; medical writing assistance from Roche and Abbvie; uncompensated advisory boards with Genentech, Roche, Daiichi-Sankyo, Seattle Genetics; compensated advisory boards with Exact Sciences; uncompensated consulting with Daiichi-Sankyo; and compensated consulting with Athenex. RC has received honoraria (outside of this study) from Amgen, Astra Zeneca, ITM, Novartis, and Scancell. BT declares stocks with Novartis; consultation fees from Eli Lilly and AstraZeneca. MCo declares research funding from Roche. PF declares travel funding from Novartis, Ipsen. MMR declares institutional research funding and/or provision of drug supply for clinical trials from Novartis, Pfizer, AstraZeneca, Roche, TerSera, Ipsen; institutional research funding from Bayer, Bristol-Myers Squibb; institutional advisory role from Ipsen; advisory role and honoraria from Bristol-Myers Squibb, Tolmar. SL receives research funding to her institution from Novartis, BMS, Merck, Roche-Genentech, Puma Biotechnology and Pfizer; consultant (not compensated) for Seattle Genetics, Pfizer, Novartis, BMS, Merck, and Roche-Genentech. All other authors have declared no conflicts of interest. Data sharing The datasets generated during and/or analysed during the current study are available on controlled access. Applications are reviewed and are approved by the IBCSG. Data access will be provided on approval to any party able to comply with the necessary agreements. This process is to comply with the ethics, legal, and data privacy obligations approved by the site ethical committees. To request access to data, contact the IBCSG Statistical Center (stat_center@ibcsg.org).
Figures
References
-
- Azim HA Jr, Michiels S, Bedard PL, et al. Elucidating prognosis and biology of breast cancer arising in young women using gene expression profiling. Clin Cancer Res. 2012;18(5):1341–1351. - PubMed
-
- Partridge AH, Hughes ME, Warner ET, et al. Subtype-dependent relationship between young age at diagnosis and breast cancer survival. J Clin Oncol. 2016;34(27):3308–3314. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- U10 CA180868/CA/NCI NIH HHS/United States
- 23916/CRUK_/Cancer Research UK/United Kingdom
- U10 CA180821/CA/NCI NIH HHS/United States
- CRUKE/03/023/CRUK_/Cancer Research UK/United Kingdom
- U24 CA075362/CA/NCI NIH HHS/United States
- U10 CA180820/CA/NCI NIH HHS/United States
- U10 CA180888/CA/NCI NIH HHS/United States
- 23433/CRUK_/Cancer Research UK/United Kingdom
- UG1 CA189867/CA/NCI NIH HHS/United States
- MR/R015724/1/MRC_/Medical Research Council/United Kingdom
- MC_PC_21026/MRC_/Medical Research Council/United Kingdom
- A15955/CRUK_/Cancer Research UK/United Kingdom
- U10 CA180863/CA/NCI NIH HHS/United States
- U10 CA180822/CA/NCI NIH HHS/United States
- CRUKE/03/022/CRUK_/Cancer Research UK/United Kingdom
- UG1 CA233328/CA/NCI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
