

Transfemoral trans-facial vein-superior ophthalmic vein to embolize cavernous sinus dural arteriovenous fistulas
- PMID: 36712416
- PMCID: PMC9877525
- DOI: 10.3389/fneur.2022.1078185
Transfemoral trans-facial vein-superior ophthalmic vein to embolize cavernous sinus dural arteriovenous fistulas
Abstract
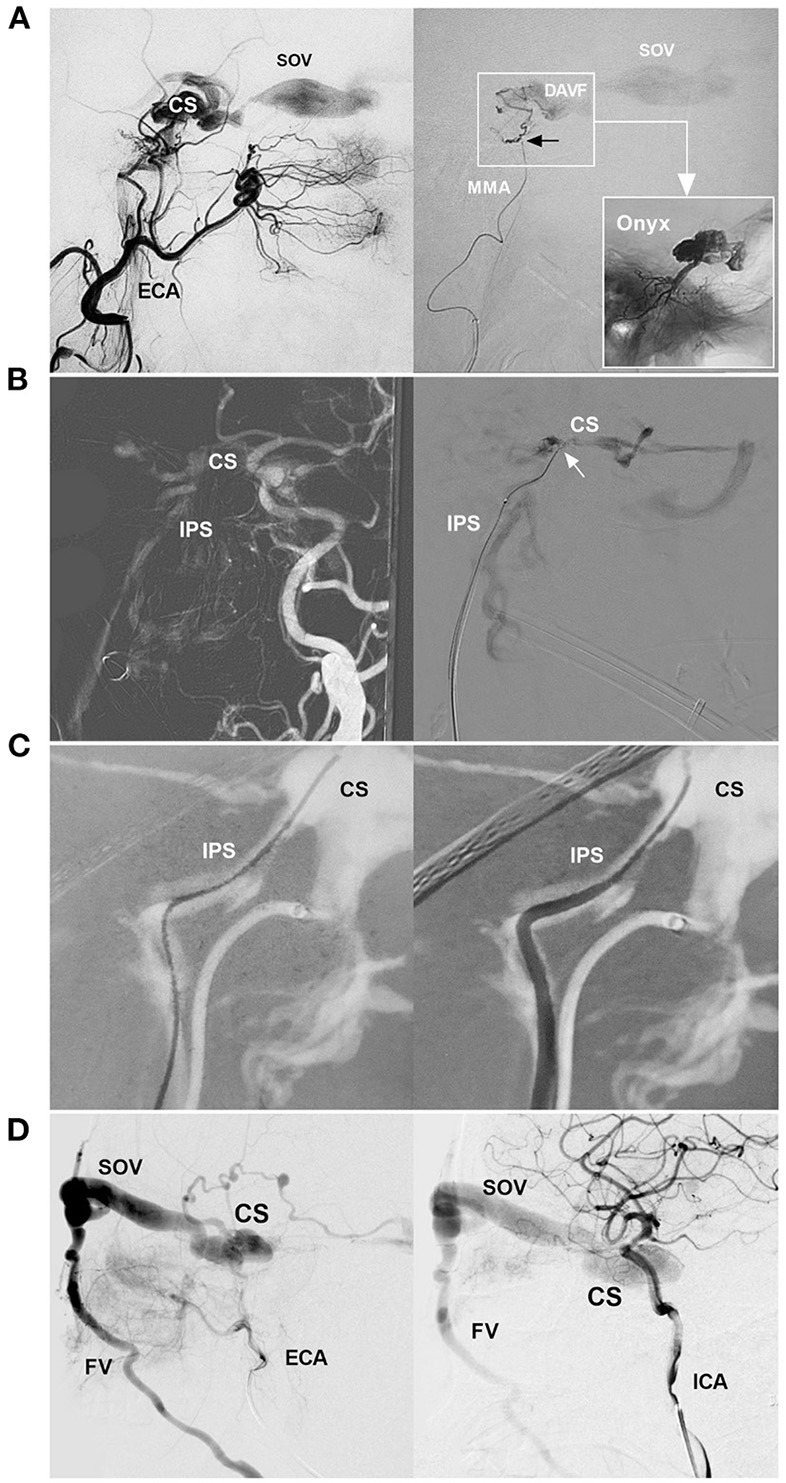
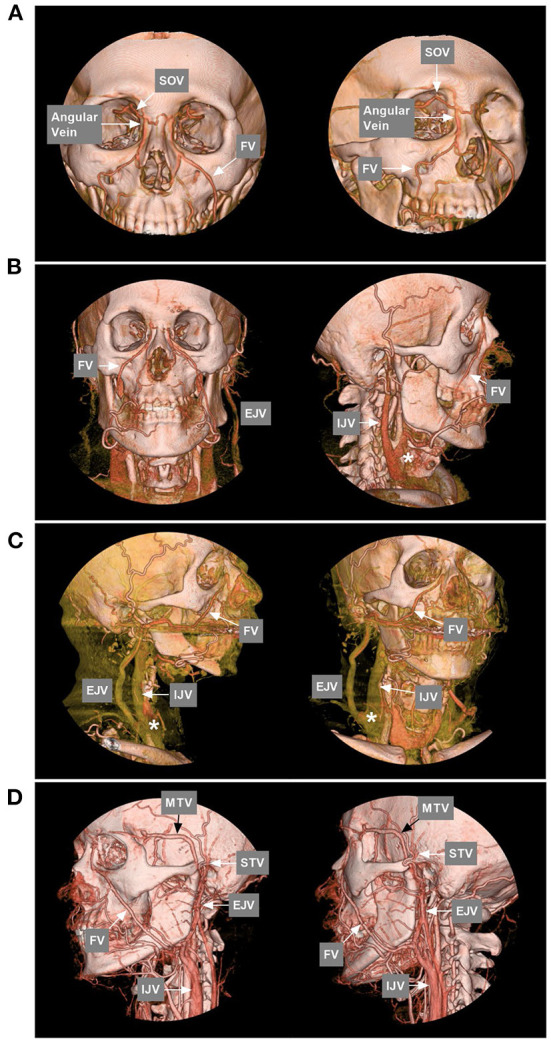
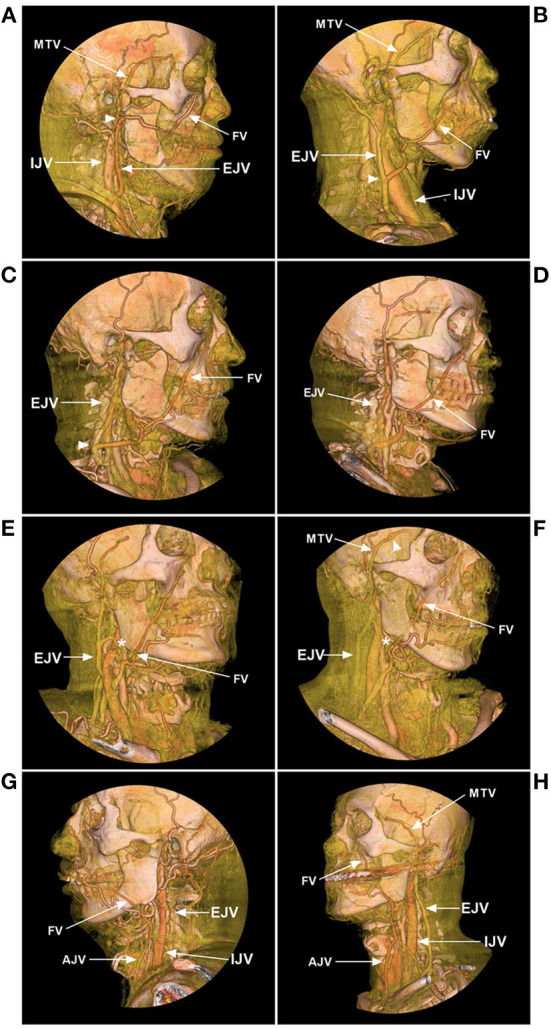
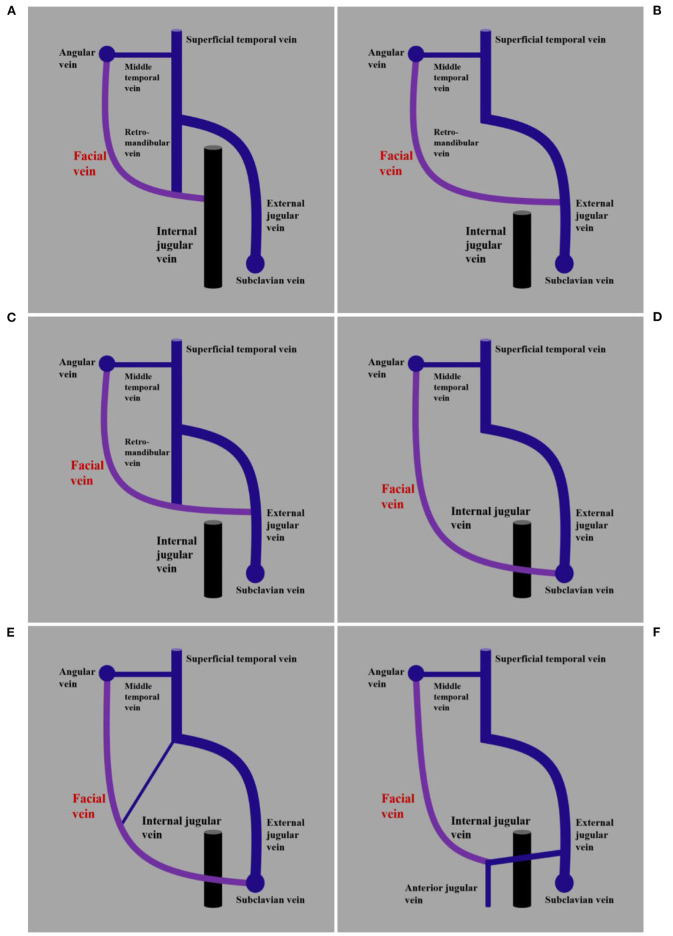
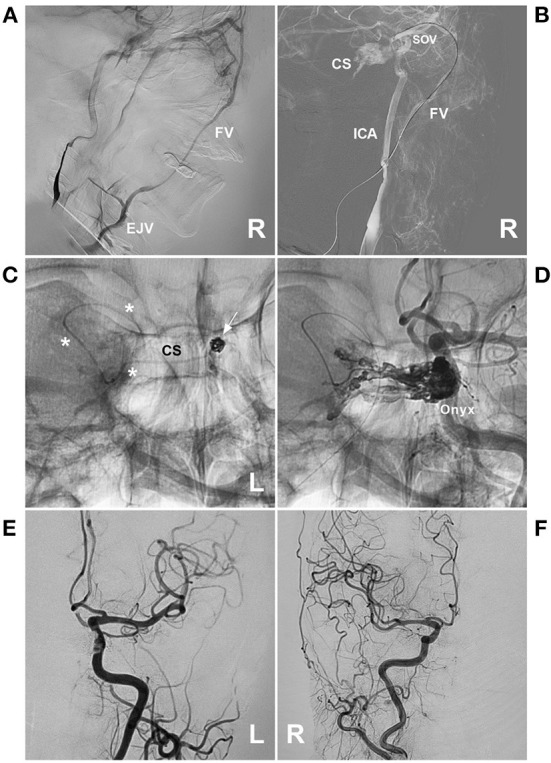
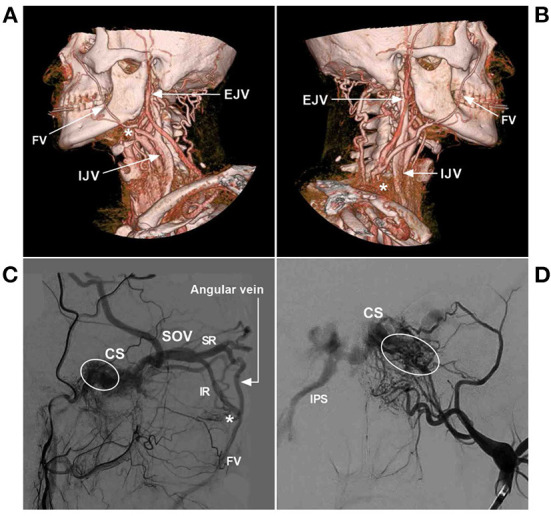
Cavernous sinus dural arteriovenous fistula (CS-DAVF) is an abnormal communication between the CS and dural arteries from the internal carotid artery and external carotid artery. CS-DAVFs are not uncommon. The preferred treatment for most CS-DAVFs is transvenous embolization (TVE), which can achieve a high cure rate with few complications. The trans-inferior petrous sinus (IPS) route from the internal jugular vein to the CS is the favorite and most direct route to perform TVE in the great majority of CS-DAVFs. However, when the trans-IPS route fails and if the facial vein (FV) is patent and dilated, transfemoral trans-FV-superior ophthalmic vein (SOV) embolization of the CS-DAVF can be attempted. However, the transfemoral trans-FV-SOV route to embolize CS-DAVFs is often challenging, and there is insufficient knowledge about it. Therefore, an updated review of the transfemoral trans-FV-SOV route to embolize CS-DAVFs is necessary, and this review includes our experience. The images in this review are from our institute without the dispute of copyright. Issues regarding the transfemoral trans-FV-SOV route to embolize CS-DAV were discussed, including the FV anatomy and variation, various TVE routes to access CS-DAVF, the procedure of the transfemoral trans-FV-SOV route to embolize CS-DAVF, difficulty, and solution of the transfemoral trans-FV-SOV route to embolize CS-DAVF, and complications and prognosis of transfemoral trans-FV-SOV to embolize CS-DAVF. By reviewing the transfemoral trans-FV-SOV route to embolize CS-DAVFs, we found that this route provides a valuable alternative to the other transvenous routes. A good prognosis can be obtained with the transfemoral trans-FV-SOV route to embolize CS-DAVFs in select cases.
Keywords: cavernous sinus; dural arteriovenous fistula; embolization; facial vein; review.
Copyright © 2023 Zhou, Xu and Yu.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources