

Eosinophilia attention, diagnosis, treatment, and awareness in physicians: a cross-sectional survey
- PMID: 36712467
- PMCID: PMC9880572
- DOI: 10.1177/20406223221146938
Eosinophilia attention, diagnosis, treatment, and awareness in physicians: a cross-sectional survey
Abstract
Background: Patients with incidental eosinophilia is becoming increasingly common in clinical practice. But it remains challenging to diagnose and treat owing to its complex etiology. The awareness of physicians and the strategies of diagnosis and treatment toward eosinophilia are still unclear.
Objective: We aimed to evaluate attention, diagnosis, treatment, and awareness of eosinophilia among physicians, as well as factors influencing clinical practice, and to find ways to improve the efficacy of this disease.
Design: This is a cross-sectional survey.
Methods: A cross-sectional study was conducted from 1 to 4 June 2021 in a tertiary hospital. Self-administered and validated electronic questionnaire was used to investigate the attention toward eosinophilia, the strategies of diagnosis and treatment, and the awareness in physicians.
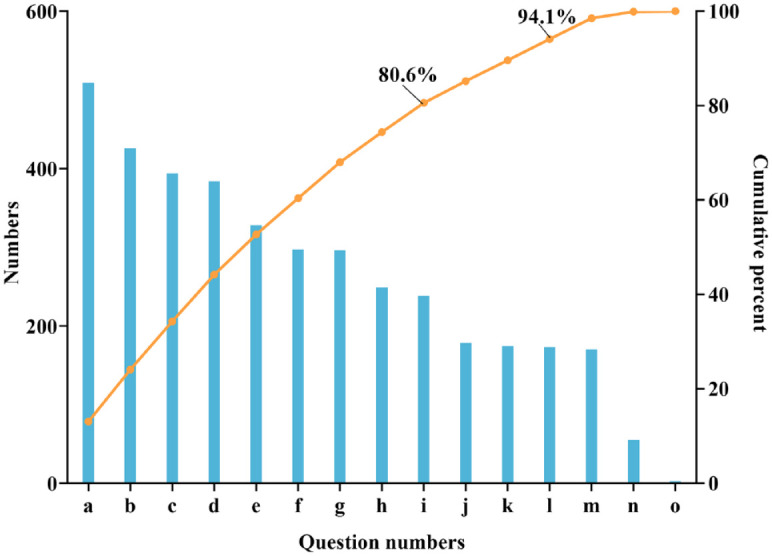
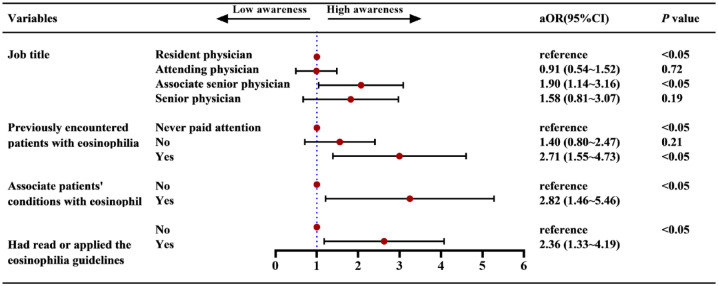
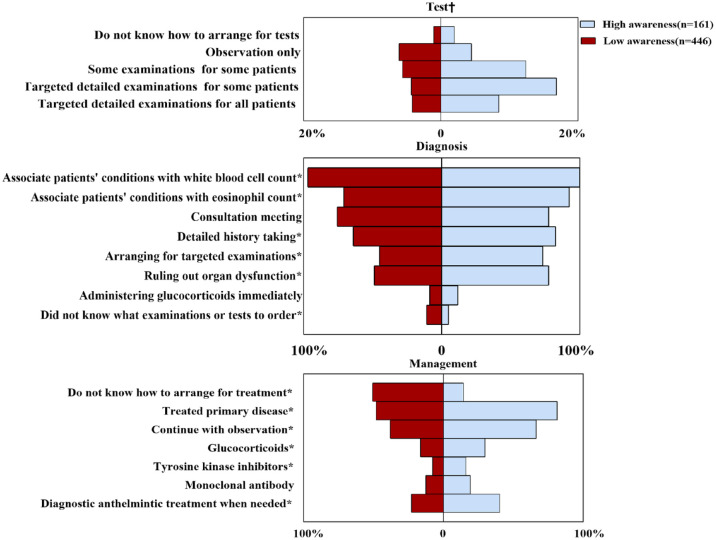
Results: A total of 607 valid questionnaires were collected, with a response rate of 84.5%. Among the responders, 65.4% of physicians claimed to be familiar with patients with eosinophilia but only 11.0% of them had read the relevant guidelines or expert consensus. Among 207 physicians who had ever diagnosed patients with eosinophilia, only 19.4% had performed detailed examinations. The accuracy of awareness questions was 1.6-53.5%, and only 26.5% of physicians had high levels of awareness. An increase in the awareness level of up to 2.82 folds was seen among physicians with factors such as job title, encountering patients with eosinophilia, linking patients' conditions to peripheral blood eosinophil count, and paying attention to guidelines.
Conclusion: This study highlighted the importance of raising awareness and knowledge of eosinophilia among physicians in China. More works on education about eosinophilia guideline are needed, which may help physicians make decision with more benefits to patients.
Keywords: attention; awareness; diagnosis; eosinophilia; questionnaire.
© The Author(s), 2023.
Conflict of interest statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures



References
-
- Shomali W, Gotlib J. World Health Organization-defined eosinophilic disorders: 2022 update on diagnosis, risk stratification, and management. Am J Hematol 2022; 97: 129–148. - PubMed
-
- Tefferi A, Patnaik MM, Pardanani A. Eosinophilia: secondary, clonal and idiopathic. Br J Haematol 2006; 133: 468–492. - PubMed
-
- Moller D, Tan J, Gauiran DTV, et al.. Causes of hypereosinophilia in 100 consecutive patients. Eur J Haematol 2020; 105: 292–301. - PubMed
-
- Hogan SP, Rosenberg HF, Moqbel R, et al.. Eosinophils: biological properties and role in health and disease. Clin Exp Allergy 2008; 38: 709–750. - PubMed
LinkOut - more resources
Full Text Sources
Medical
