

Usefulness of a laser-cut covered metal stent with a 7F delivery sheath in endoscopic ultrasound-guided biliary drainage without fistula dilation
- PMID: 36712906
- PMCID: PMC9879640
- DOI: 10.1055/a-1997-9149
Usefulness of a laser-cut covered metal stent with a 7F delivery sheath in endoscopic ultrasound-guided biliary drainage without fistula dilation
Abstract
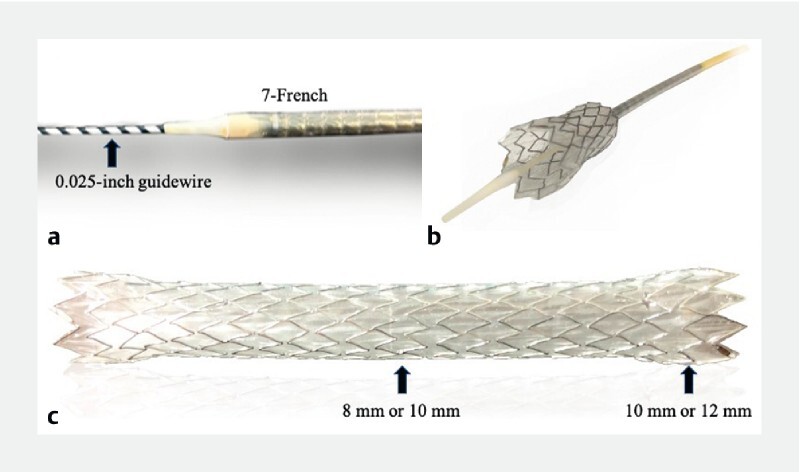
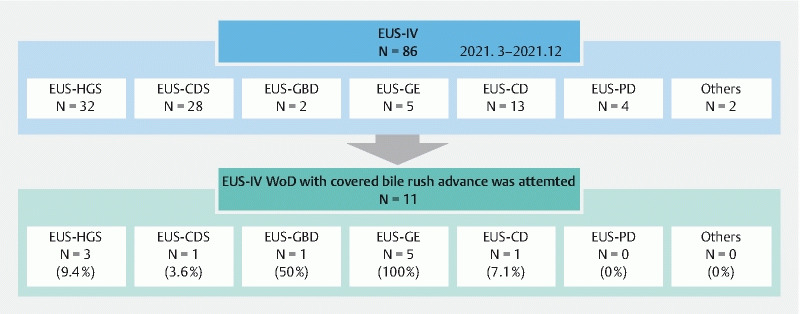
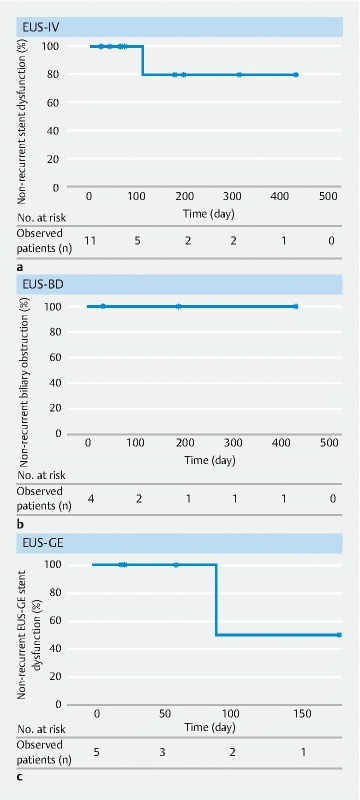
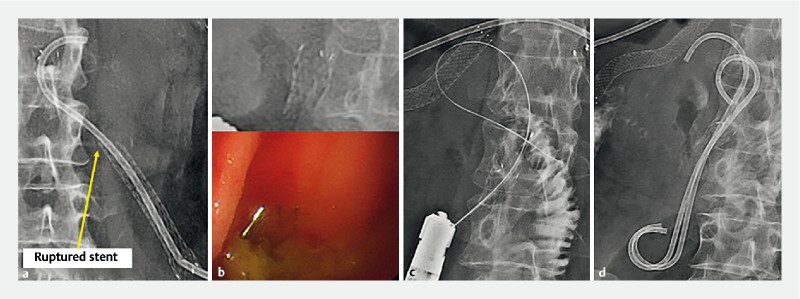
Background and study aims Recently, the utility of endoscopic ultrasound-guided intervention without fistula dilation (EUS-IV WoD) has been reported to prevent adverse events. We clinically evaluated cases in which EUS-IV WoD was attempted using a novel self-expandable metallic stent (SEMS); this is a fully covered, laser-cut SEMS that has a tapered and stiff tip specifically designed for a 0.025-inch guidewire and a relatively thin, 7F delivery system. Patients and methods We retrospectively evaluated cases wherein EUS-IV WoD was attempted using the novel SEMS between March and December 2021. Results Treatment of 11 patients by EUS-IV WoD with the novel SEMS was attempted. The technical success rate for EUS-IV was 100 % and the clinical success rate was 100 %; the success rate for EUS-IV WoD was 72.8 %. Of these, the procedural success rate for EUS-IV WoD was 100 % in EUS-biliary drainage (BD) and 57.1 % in non-EUS-BD. Early adverse events were observed in 27.3 % of patients (3/11): mild abdominal pain in two patients and moderate bleeding in one patient. The abdominal pain cases were both cases of EUS-IV WoD failure and required fistula dilation. Conclusions The novel stent may be useful for EUS-IV WoD, especially in EUS-BD.
The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/).
Conflict of interest statement
Competing interests The authors declare that they have no conflict of interest.
Figures
References
-
- Moss A C, Morris E, Leyden J et al. Do the benefits of metal stents justify the costs? A systematic review and meta-analysis of trials comparing endoscopic stents for malignant biliary obstruction. Eur J Gastroenterol Hepatol. 2007;19:1119–1124. - PubMed
-
- Park D H, Lee T H, Paik W H et al. Feasibility and safety of a novel dedicated device for one-step EUS-guided biliary drainage: a randomized trial. J Gastroenterol Hepatol. 2015;30:1461–1466. - PubMed
-
- Itonaga M, Kitano M, Hatamaru K et al. Endoscopic ultrasound-guided choledochoduodenostomy using a thin stent delivery system in patients with unresectable malignant distal biliary obstruction: a prospective multicenter study. Dig Endosc. 2019;31:291–298. - PubMed
LinkOut - more resources
Full Text Sources