

Universal Clinician Device for improving risk prediction and management of patients with atrial fibrillation: an assumed benefit analysis
- PMID: 36713019
- PMCID: PMC9707904
- DOI: 10.1093/ehjdh/ztac011
Universal Clinician Device for improving risk prediction and management of patients with atrial fibrillation: an assumed benefit analysis
Abstract
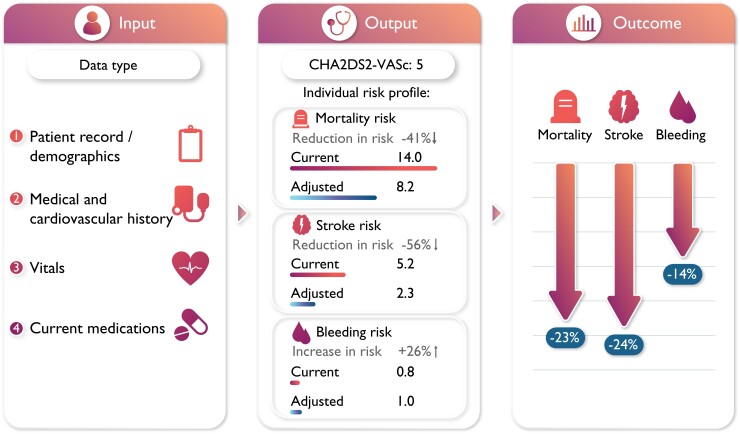
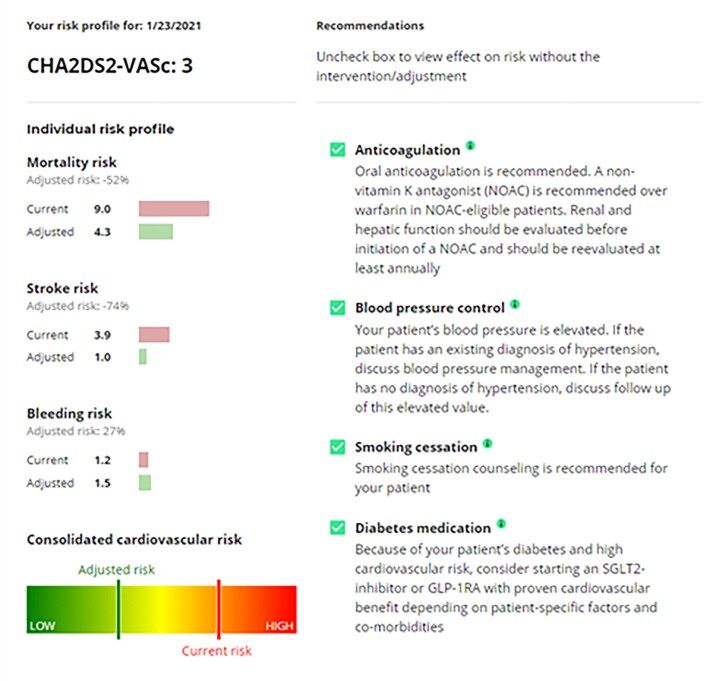
Aim: Atrial fibrillation (AF) management guidelines advise using risk tools to optimize AF treatment. This study aims to develop a dynamic and clinically applicable digital device to assess stroke and bleeding risk, and to facilitate outcome improvements in AF patients. The device will provide tailored treatment recommendations according to easily attainable individual patient data.
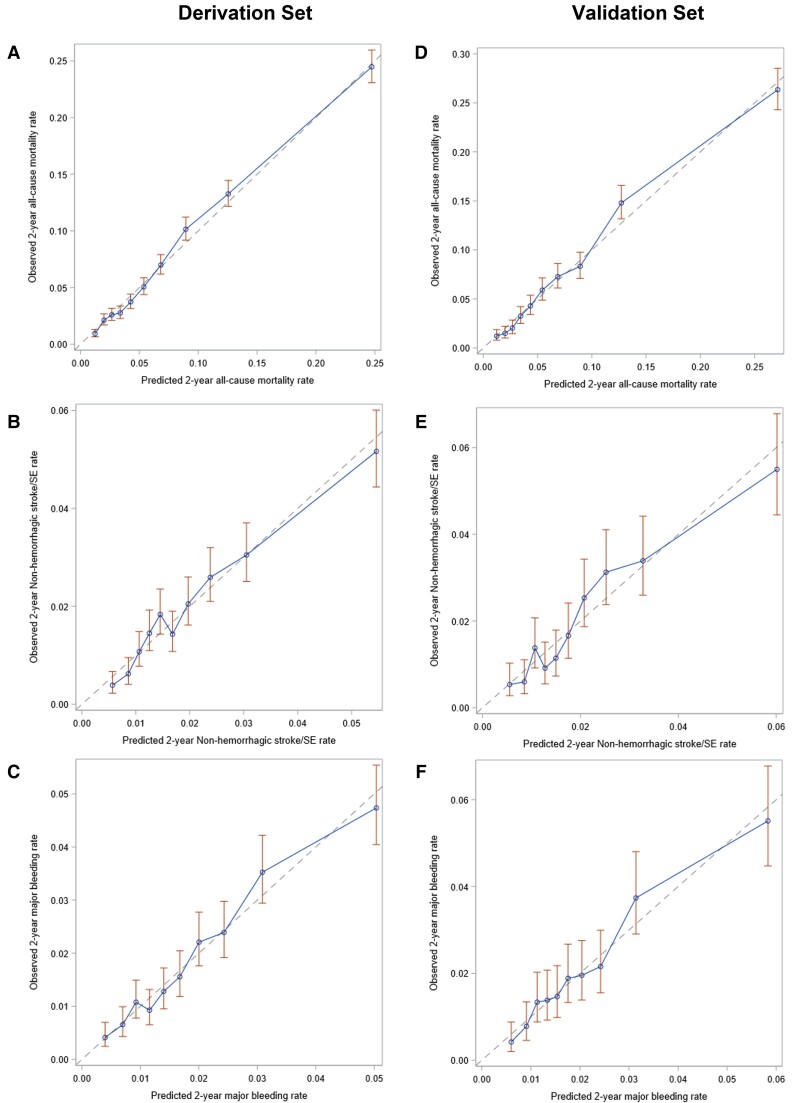
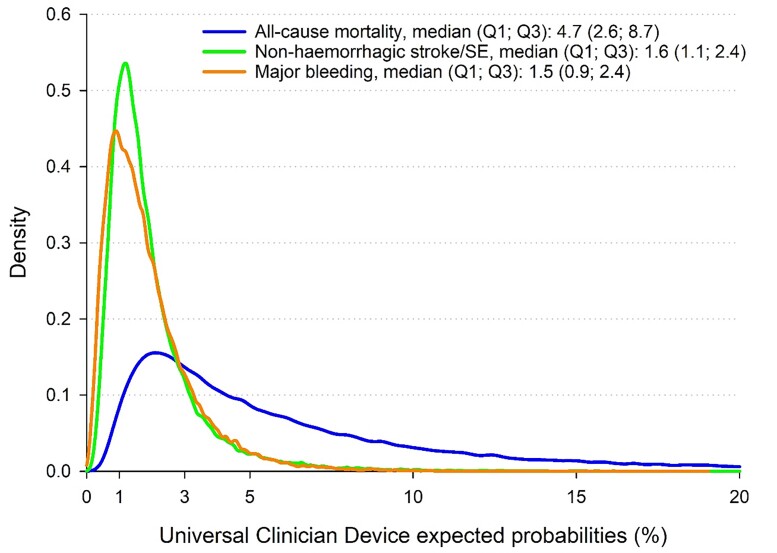
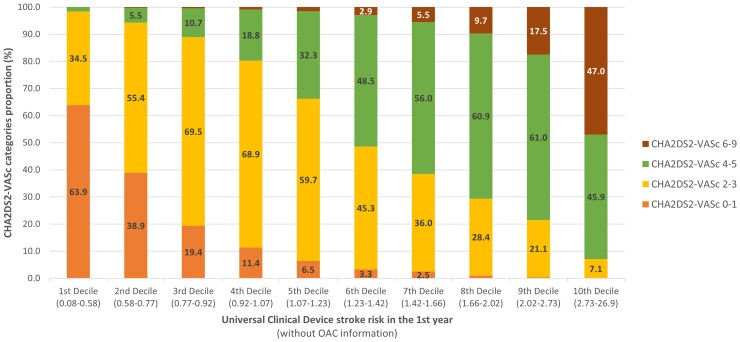
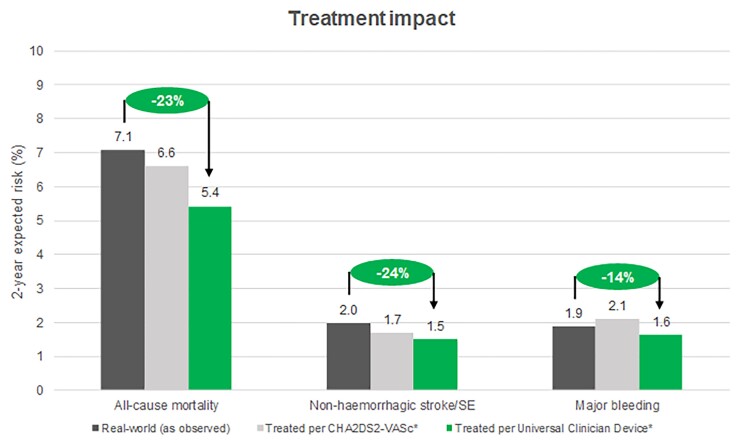
Methods and results: This Universal Clinician Device (UCD) was created using the GARFIELD-AF registry using a split sample approach. The GARFIELD-AF risk tool was adapted with two modifications. First, predictors with ≥1000 missing data points were separated, allowing expected risks estimation. Second, recommendations for modifiable risk factors and associated 2-year outcome estimates were incorporated. Outcomes of interest were all-cause mortality, non-haemorrhagic stroke/systemic embolism (SE), and major bleeding. All patients were randomized to a derivation (n = 34853) and validation cohort (n = 17165). In the derivation cohort, predictors were identified using least absolute shrinkage and selection operator regression. Cox models were fitted with the selected parameters. The UCD demonstrated superior predictive power compared with CHA2DS2VASc for all-cause mortality [0.75(0.75-0.76) vs. 0.71(0.70-0.72)] and non-haemorrhagic stroke/SE [0.68(0.66-0.70) vs. 0.65(0.63-0.67)], and with HAS-BLED for major bleeding [0.69(0.67-0.71) vs. 0.64(0.62-0.65)]. Universal Clinician Device recommendations reduced all-cause mortality (8.45-5.42%) and non-haemorrhagic stroke/SE (2.58-1.50%). Patients with concomitant diabetes and chronic kidney disease benefitted further, reducing mortality risk from 13.15% to 8.67%. One-third of patients with a CHA2DS2VASc score of >1 had the lowest risk of stroke.
Conclusion: The UCD simultaneously predicts mortality, stroke, and bleeding risk in patients using easily attainable individual clinical data and guideline-based optimized treatment plans.
Clinical trial registration: URL: http://www.clinicaltrials.gov. Unique identifier for GARFIELD-AF: NCT01090362.
Keywords: Atrial fibrillation; Diabetes; Management guidelines; Personalized medicine; Risk prediction; Universal Clinician Device.
© The Author(s) 2022. Published by Oxford University Press on behalf of European Society of Cardiology.
Figures
References
-
- Lippi G, Sanchis-Gomar F, Cervellin G. Global epidemiology of atrial fibrillation: an increasing epidemic and public health challenge. Int J Stroke 2021;16(2):217–221. - PubMed
-
- Friberg L, Hammar N, Ringh M, Pettersson H, Rosenqvist M. Stroke prophylaxis in atrial fibrillation: who gets it and who does not? Report from the Stockholm Cohort-study on Atrial Fibrillation (SCAF-study). Eur Heart J 2006;27:1954–1964. - PubMed
-
- Stewart S, Hart CL, Hole DJ, McMurray JJ. A population-based study of the long-term risks associated with atrial fibrillation: 20-year follow-up of the Renfrew/Paisley study. Am J Med 2002;113:359–364. - PubMed
-
- Christiansen CB, Gerds TA, Olesen JB, Kristensen SL, Lamberts M, Lip GYH, Gislason GH, Køber L, Torp-Pedersen C. Atrial fibrillation and risk of stroke: a nationwide cohort study. Europace 2016;18:1689–1697. - PubMed
-
- Boston Area Anticoagulation Trial for Atrial Fibrillation Investigators, Singer DE, Hughes RA, Gress DR, Sheehan MA, Oertel LB, Maraventano SW, Blewett DR, Rosner B, Kistler JP. The effect of low-dose warfarin on the risk of stroke in patients with nonrheumatic atrial fibrillation. N Engl J Med 1990;323:1505–1511. - PubMed
Associated data
LinkOut - more resources
Full Text Sources
Medical