

Case report: Daratumumab for treatment of refractory late or chronic active antibody-mediated rejection in renal allograft recipients with high levels of de novo donor-specific antibodies
- PMID: 36713391
- PMCID: PMC9875042
- DOI: 10.3389/fimmu.2022.1087597
Case report: Daratumumab for treatment of refractory late or chronic active antibody-mediated rejection in renal allograft recipients with high levels of de novo donor-specific antibodies
Abstract
Background: Late or chronic active antibody-mediated rejection (AMR) associated with de novo donor-specific antibodies (dnDSA) after renal transplantation is a great clinical challenge because it is often resistant to conventional therapies. Daratumumab, an anti-CD38 monoclonal antibody that can deplete plasma cells, may be effective for the treatment of late or chronic active AMR.
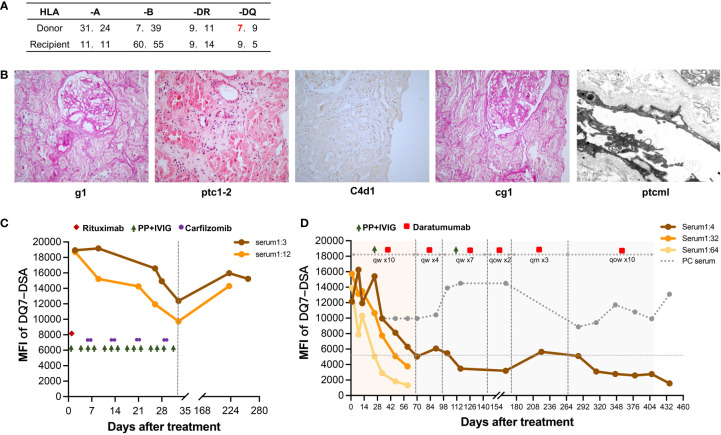
Methods: We designed a novel regimen that included early intensive therapy with daratumumab plus plasmapheresis (PP)/intravenous immunoglobulins (IVIG) and later maintenance therapy with daratumumab alone, and used this regimen to treat late or chronic active AMR in two kidney transplant recipients with extremely high levels of anti-DQ7 dnDSA.
Results: Both patients had a limited clinical response to the early treatment with rituximab and PP/IVIG (with or without splenic irradiation); however, they had a remarkable decrease in anti-DQ7 DSA (MFI value from ~20,000 to ~5,000) after 2-3 months of intensive therapy with daratumumab plus PP/IVIG. Over 20 months of follow-up, patient 1 maintained a low DSA (as low as 1,572) and normal renal function on daratumumab maintenance therapy. Patient 2 retained a low DSA and improved renal function and pathological lesions within one year after treatment but then deteriorated because of acute T cell-mediated rejection.
Conclusions: Our daratumumab-based regimen has shown promising results in the treatment of refractory late active or chronic active AMR in renal transplant recipients with high-level dnDSA. This may provide a reference for better use of daratumumab in the treatment of late or chronic active AMR.
Keywords: HLA-DQ; case report; chronic active antibody-mediated rejection; daratumumab; donor specific antibodies; kidney transplantation.
Copyright © 2023 Zhu, Guo, Zhao, Sa, Zhao, Guo and Chen.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures


References
-
- Moreso F, Crespo M, Ruiz JC, Torres A, Gutierrez-Dalmau A, Osuna A, et al. . Treatment of chronic antibody mediated rejection with intravenous immunoglobulins and rituximab: A multicenter, prospective, randomized, double-blind clinical trial. Am J Transplant (2018) 18(4):927–35. doi: 10.1111/ajt.14520 - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous