

The clinical outcomes of imaging modalities for surgical management Cushing's disease - A systematic review and meta-analysis
- PMID: 36714581
- PMCID: PMC9880448
- DOI: 10.3389/fendo.2022.1090144
The clinical outcomes of imaging modalities for surgical management Cushing's disease - A systematic review and meta-analysis
Abstract
Introduction: Cushing's disease presents major diagnostic and management challenges. Although numerous preoperative and intraoperative imaging modalities have been deployed, it is unclear whether these investigations have improved surgical outcomes. Our objective was to investigate whether advances in imaging improved outcomes for Cushing's disease.
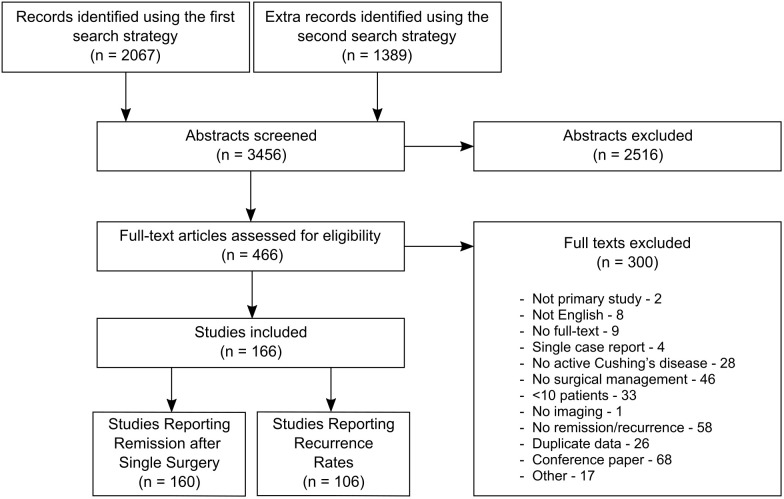
Methods: Searches of PubMed and EMBASE were conducted. Studies reporting on imaging modalities and clinical outcomes after surgical management of Cushing's disease were included. Multilevel multivariable meta-regressions identified predictors of outcomes, adjusting for confounders and heterogeneity prior to investigating the effects of imaging.
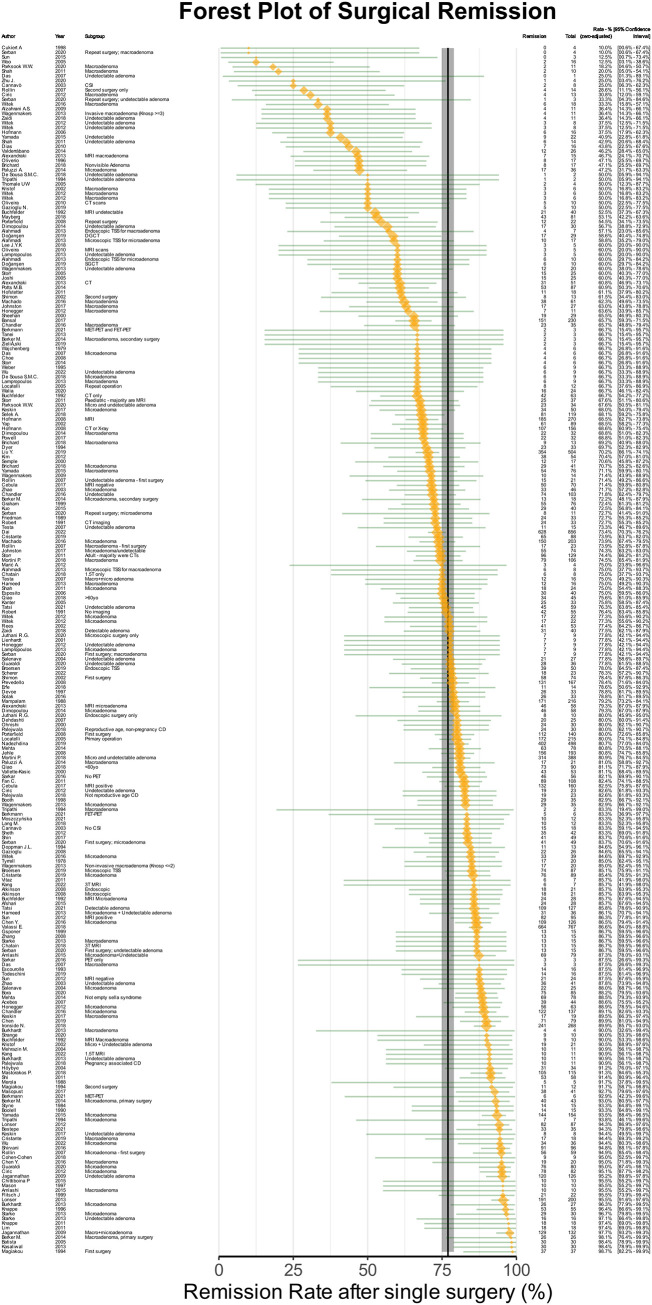
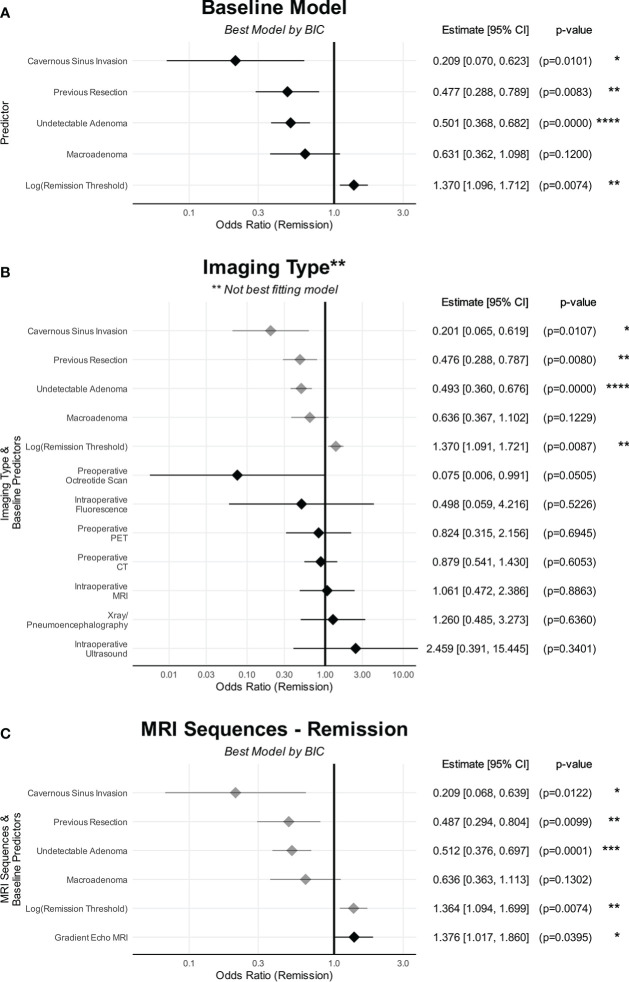
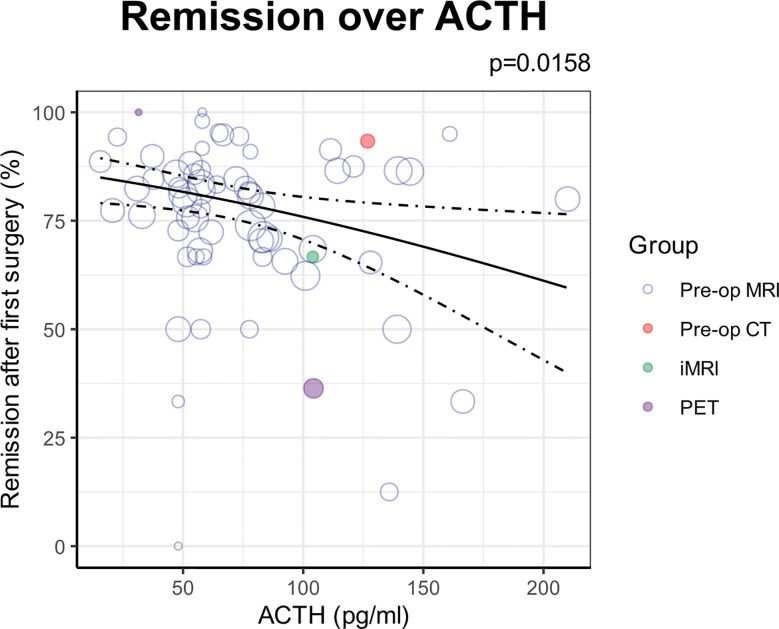
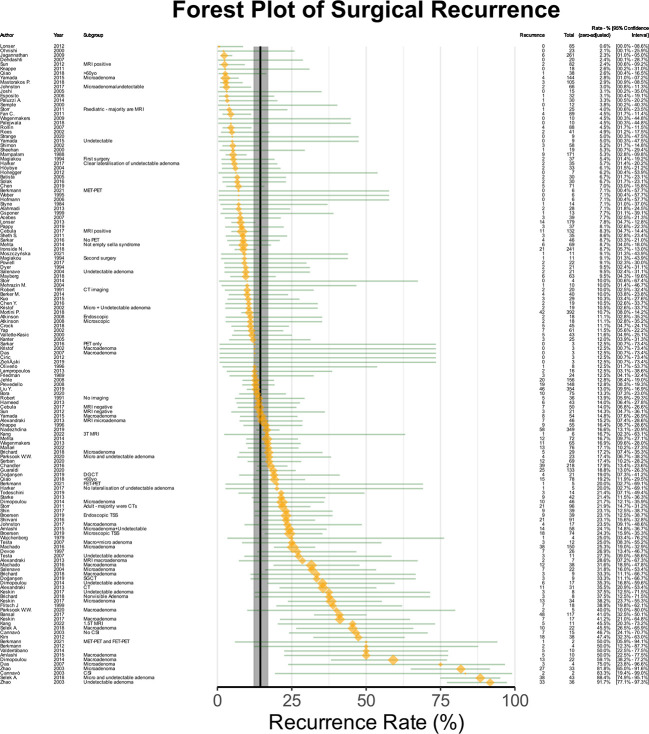
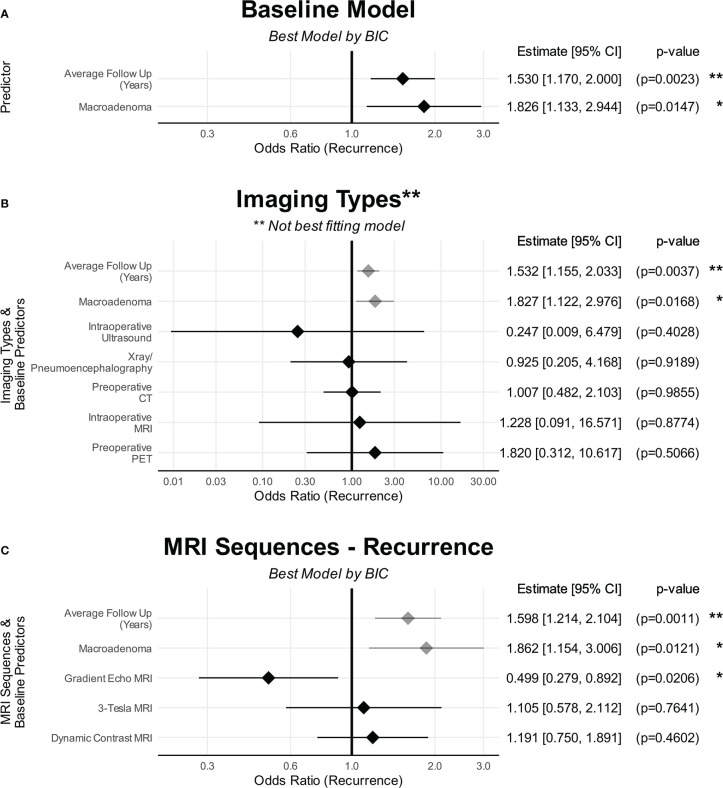
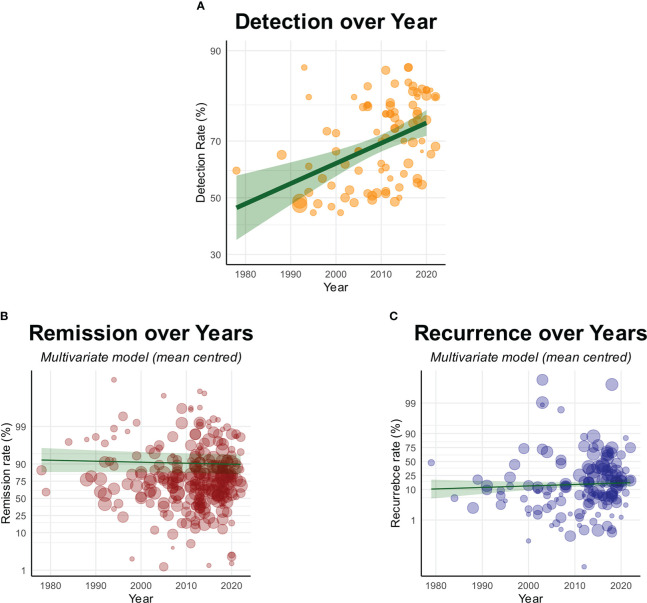
Results: 166 non-controlled single-arm studies were included, comprising 13181 patients over 44 years.The overall remission rate was 77.0% [CI: 74.9%-79.0%]. Cavernous sinus invasion (OR: 0.21 [CI: 0.07-0.66]; p=0.010), radiologically undetectable lesions (OR: 0.50 [CI: 0.37-0.69]; p<0.0001), previous surgery (OR=0.48 [CI: 0.28-0.81]; p=0.008), and lesions ≥10mm (OR: 0.63 [CI: 0.35-1.14]; p=0.12) were associated with lower remission. Less stringent thresholds for remission was associated with higher reported remission (OR: 1.37 [CI: 1.1-1.72]; p=0.007). After adjusting for this heterogeneity, no imaging modality showed significant differences in remission compared to standard preoperative MRI.The overall recurrence rate was 14.5% [CI: 12.1%-17.1%]. Lesion ≥10mm was associated with greater recurrence (OR: 1.83 [CI: 1.13-2.96]; p=0.015), as was greater duration of follow-up (OR: 1.53 (CI: 1.17-2.01); p=0.002). No imaging modality was associated with significant differences in recurrence.Despite significant improvements in detection rates over four decades, there were no significant changes in the reported remission or recurrence rates.
Conclusion: A lack of controlled comparative studies makes it difficult to draw definitive conclusions. Within this limitation, the results suggest that despite improvements in radiological detection rates of Cushing's disease over the last four decades, there were no changes in clinical outcomes. Advances in imaging alone may be insufficient to improve surgical outcomes.
Systematic review registration: https://www.crd.york.ac.uk/PROSPERO/, identifier CRD42020187751.
Keywords: Cushing’s disease; MRI; PET; advanced imaging; cushing; imaging; pituitary; transsphenoidal.
Copyright © 2023 Koh, Khan, Digpal, Layard Horsfall, Ali, Baldeweg, Bouloux, Dorward, Drake, Evanson, Grieve, Stoyanov, Korbonits and Marcus.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Ghorbani M, Akbari H, Griessenauer CJ, Wipplinger C, Dastmalchi A, Malek M, et al. Lateralization of inferior petrosal sinus sampling in cushing’s disease correlates with cavernous sinus venous drainage patterns, but not tumor lateralization. Heliyon (2020) 6(10):e05299. doi: 10.1016/j.heliyon.2020.e05299 - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources