

Heart-gut microbiota communication determines the severity of cardiac injury after myocardial ischaemia/reperfusion
- PMID: 36715640
- PMCID: PMC10262181
- DOI: 10.1093/cvr/cvad023
Heart-gut microbiota communication determines the severity of cardiac injury after myocardial ischaemia/reperfusion
Abstract
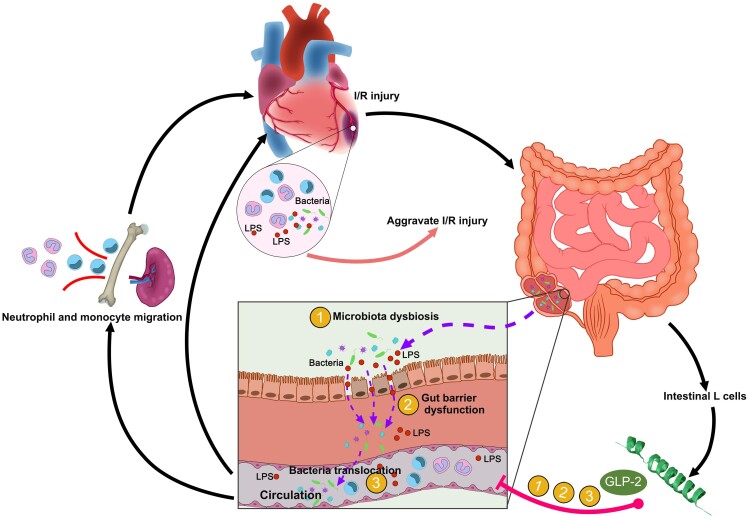
Aims: Recent studies have suggested a key role of intestinal microbiota in pathological progress of multiple organs via immune modulation. However, the interactions between heart and gut microbiota remain to be fully elucidated. The aim of the study is to investigate the role of gut microbiota in the post-ischaemia/reperfusion (I/R) inflammatory microenvironment.
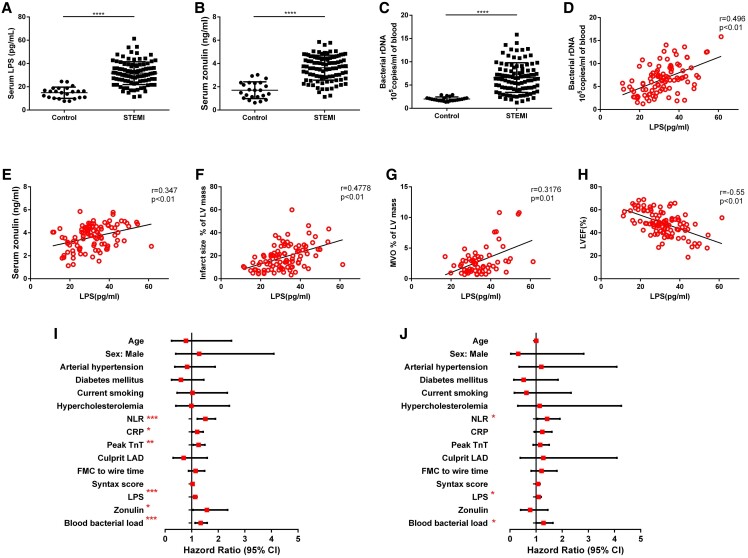
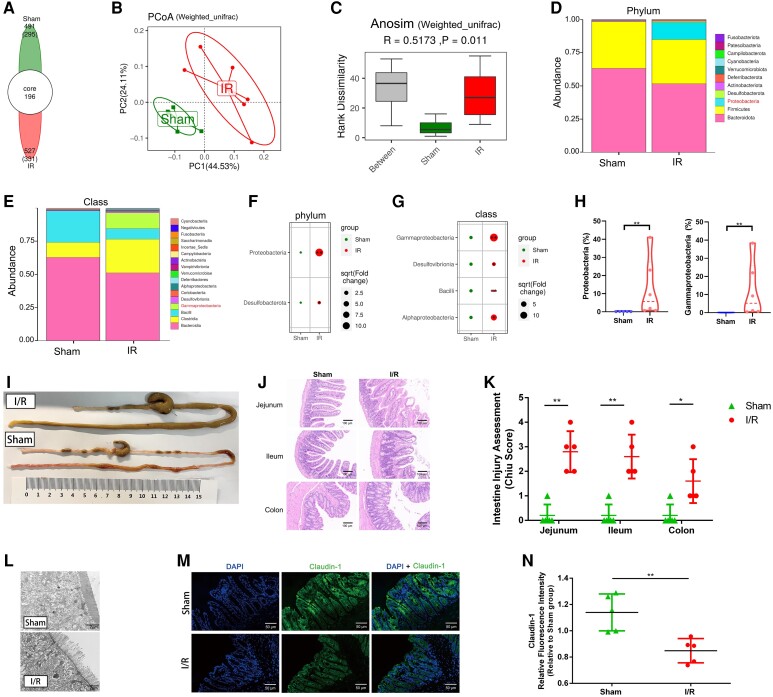
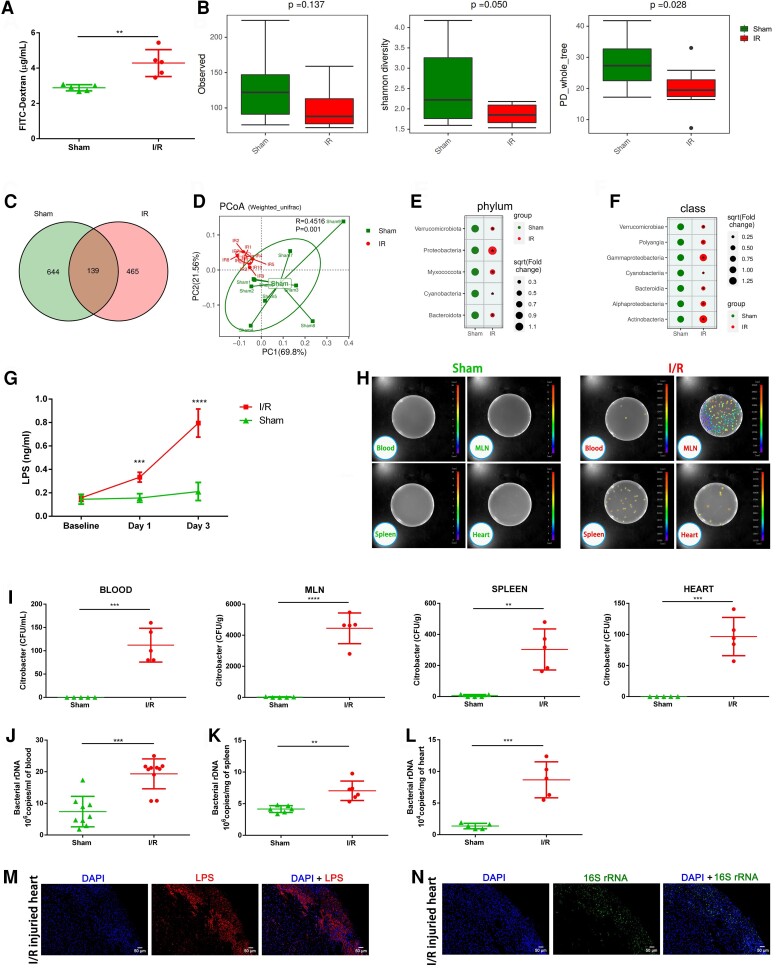
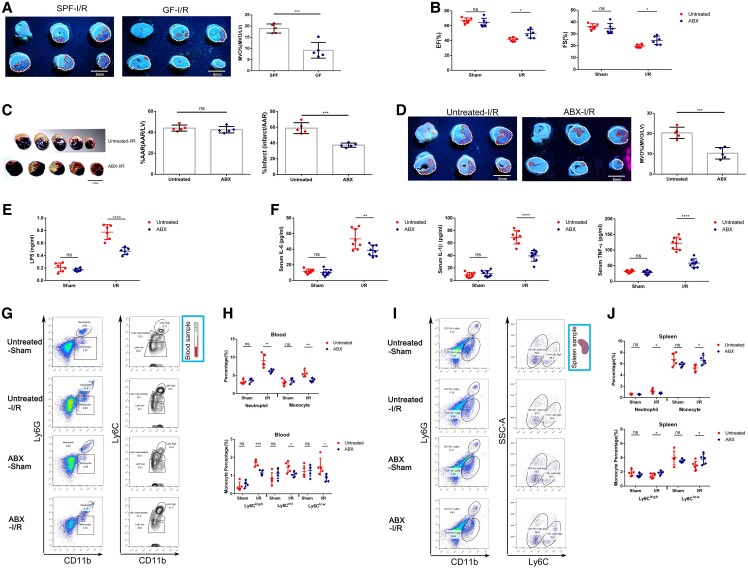
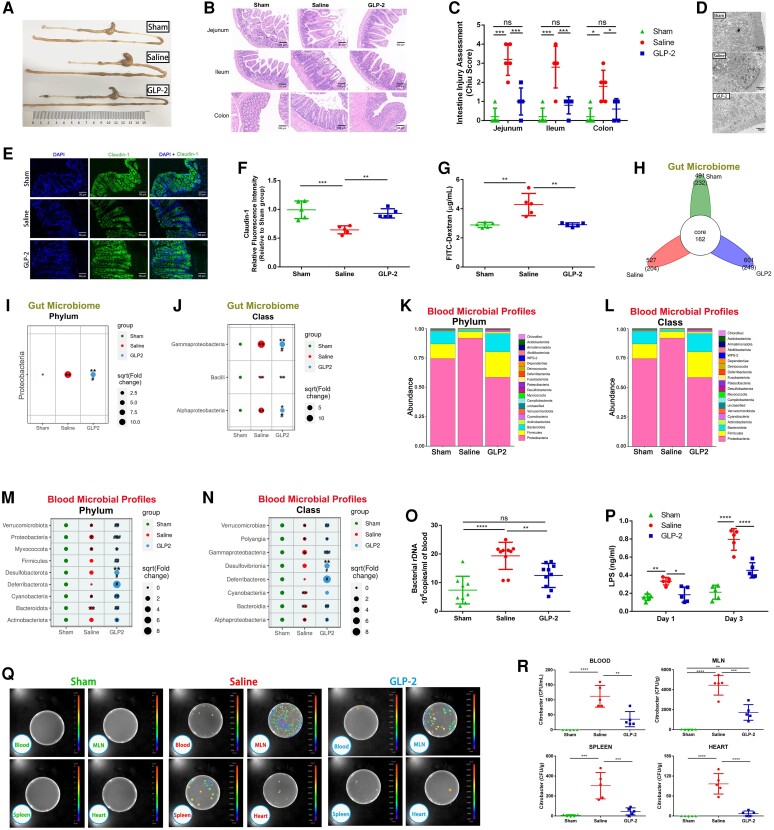
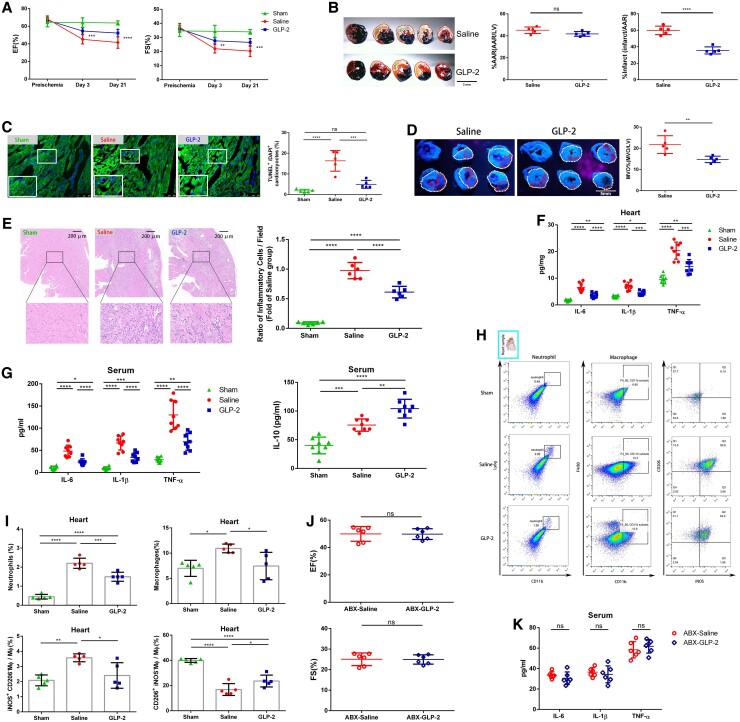
Methods and results: Here, we conducted a case-control study to explore the association of gut bacteria translocation products with inflammation biomarkers and I/R injury severity in ST-elevation myocardial infarction patients. Then, we used a mouse model to determine the effects of myocardial I/R injury on gut microbiota dysbiosis and translocation. Blooming of Proteobacteria was identified as a hallmark of post-I/R dysbiosis, which was associated with gut bacteria translocation. Abrogation of gut bacteria translocation by antibiotic cocktail alleviated myocardial I/R injury via mitigating excessive inflammation and attenuating myeloid cells mobilization, indicating the bidirectional heart-gut-microbiome-immune axis in myocardial I/R injury. Glucagon-like peptide 2 (GLP-2), an endocrine peptide produced by intestinal L-cells, was used in the experimental myocardial I/R model. GLP-2 administration restored gut microbiota disorder and prevented bacteria translocation, eventually attenuated myocardial I/R injury through alleviating systemic inflammation.
Conclusion: Our work identifies a bidirectional communication along the heart-gut-microbiome-immune axis in myocardial I/R injury and demonstrates gut bacteria translocation as a key regulator in amplifying inflammatory injury. Furthermore, our study sheds new light on the application of GLP-2 as a promising therapy targeting gut bacteria translocation in myocardial I/R injury.
Keywords: Bacteria translocation; Glucagon-like peptide 2; Gut microbiota dysbiosis; Inflammation; Myocardial ischaemia/reperfusion injury.
© The Author(s) 2023. Published by Oxford University Press on behalf of the European Society of Cardiology.
Conflict of interest statement
Conflict of interest: None declared.
Figures
References
-
- Heusch G. Myocardial ischaemia–reperfusion injury and cardioprotection in perspective. Nat Rev Cardiol 2020;17:773–789. - PubMed
-
- Bekkers SCAM, Yazdani SK, Virmani R, Waltenberger J. Microvascular obstruction: underlying pathophysiology and clinical diagnosis. J Am Coll Cardiol 2010;55:1649–1660. - PubMed
-
- Heusch G. Coronary microvascular obstruction: the new frontier in cardioprotection. Basic Res Cardiol 2019;114:45. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
