

Should individual timeline and serial CT/MRI panels of all patients be presented in acute brain insult cohorts? A pilot study of 45 patients with decompressive craniectomy after aneurysmal subarachnoid hemorrhage
- PMID: 36715752
- PMCID: PMC10624760
- DOI: 10.1007/s00701-022-05473-7
Should individual timeline and serial CT/MRI panels of all patients be presented in acute brain insult cohorts? A pilot study of 45 patients with decompressive craniectomy after aneurysmal subarachnoid hemorrhage
Abstract
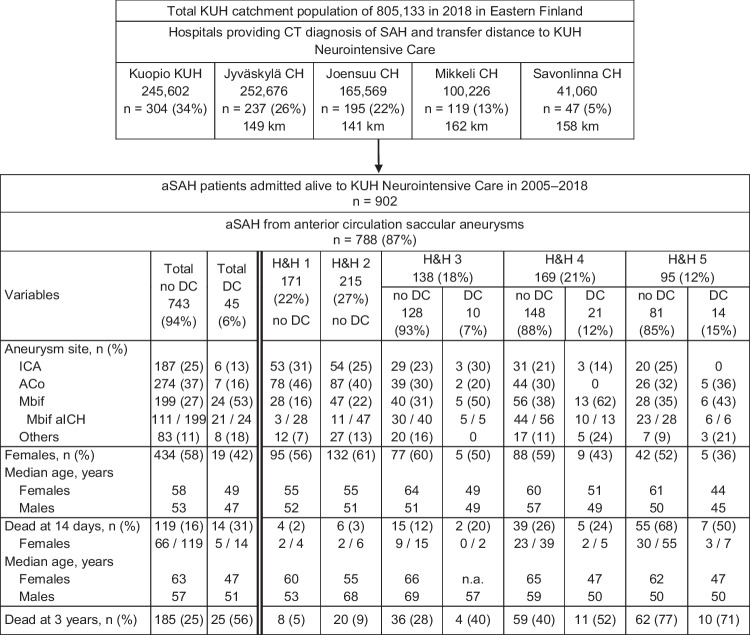
Purpose: Our review of acute brain insult articles indicated that the patients' individual (i) timeline panels with the defined time points since the emergency call and (ii) serial brain CT/MRI slice panels through the neurointensive care until death or final brain tissue outcome at 12 months or later are not presented.
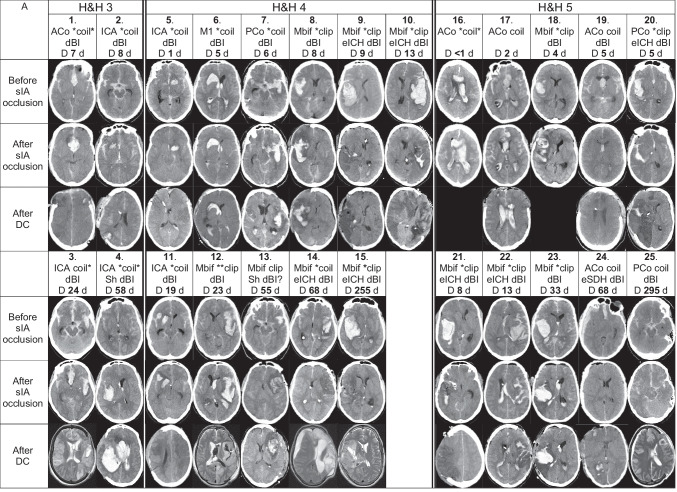
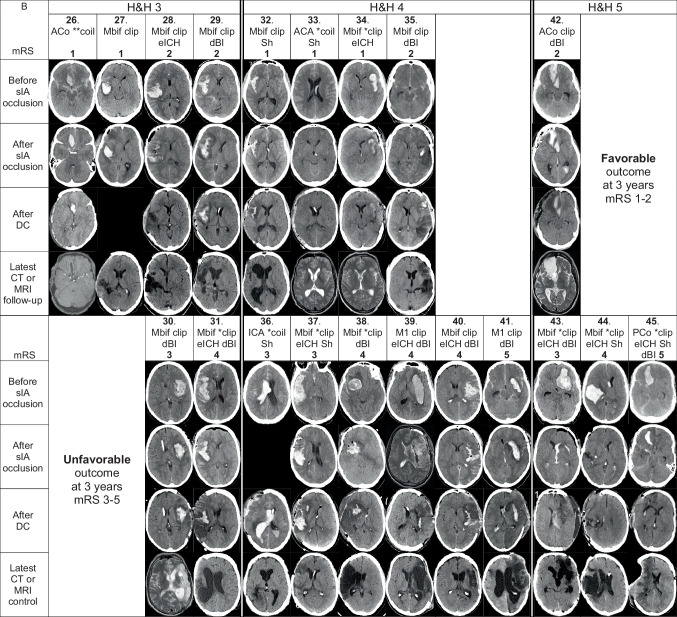
Methods: We retrospectively constructed such panels for the 45 aneurysmal subarachnoid hemorrhage (aSAH) patients with a secondary decompressive craniectomy (DC) after the acute admission to neurointensive care at Kuopio University Hospital (KUH) from a defined population from 2005 to 2018. The patients were indicated by numbers (1.-45.) in the pseudonymized panels, tables, results, and discussion. The timelines contained up to ten defined time points on a logarithmic time axis until death ([Formula: see text]; 56%) or 3 years ([Formula: see text]; 44%). The brain CT/MRI panels contained a representative slice from the following time points: SAH diagnosis, after aneurysm closure, after DC, at about 12 months (20 survivors).
Results: The timelines indicated re-bleeds and allowed to compare the times elapsed between any two time points, in terms of workflow swiftness. The serial CT/MRI slices illustrated the presence and course of intracerebral hemorrhage (ICH), perihematomal edema, intraventricular hemorrhage (IVH), hydrocephalus, delayed brain injury, and, in the 20 (44%) survivors, the brain tissue outcome.
Conclusions: The pseudonymized timeline panels and serial brain imaging panels, indicating the patients by numbers, allowed the presentation and comparison of individual clinical courses. An obvious application would be the quality control in acute or elective medicine for timely and equal access to clinical care.
Keywords: Aneurysmal subarachnoid hemorrhage; Brain tissue outcome; EMS (emergency medical services); Individual serial brain imaging panels; Individual timeline panels; Neurointensive care.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures




References
-
- Adams H, Ban VS, Leinonen V, Aoun SG, Huttunen J, Saavalainen T, Lindgren A, Frosen J, von Und Zu, Fraunberg M, Koivisto T, Hernesniemi J, Welch BG, Jääskeläinen JE, Huttunen TJ. Risk of shunting after aneurysmal subarachnoid hemorrhage: a collaborative study and initiation of a consortium. Stroke. 2016;47:2488–2496. doi: 10.1161/STROKEAHA.116.013739. - DOI - PubMed
-
- Allen JW, Prater A, Kallas O, Abidi SA, Howard BM, Tong F, Agarwal S, Yaghi S, Dehkharghani S. Diagnostic performance of computed tomography angiography and computed tomography perfusion tissue time-to-maximum in vasospasm following aneurysmal subarachnoid hemorrhage. J Am Heart Assoc. 2022 doi: 10.1161/JAHA.121.023828. - DOI - PMC - PubMed
-
- Alotaibi NM, Elkarim GA, Samuel N, Ayling OGS, Guha D, Fallah A, Aldakkan A, Jaja BNR, de Oliveira Manoel AL, Ibrahim GM, Macdonald RL. Effects of decompressive craniectomy on functional outcomes and death in poor-grade aneurysmal subarachnoid hemorrhage: a systematic review and meta-analysis. J Neurosurg. 2017;127:1315–1325. doi: 10.3171/2016.9.JNS161383. - DOI - PubMed
-
- Autio AH, Paavola J, Tervonen J, Lång M, Huuskonen TJ, Huttunen J, Kärkkäinen V, von Und Zu, Fraunberg M, Lindgren AE, Koivisto T, Jääskeläinen JE, Kämäräinen OP. Clinical condition of 120 patients alive at 3 years after poor-grade aneurysmal subarachnoid hemorrhage. Acta Neurochir. 2021;163:1153–1166. doi: 10.1007/s00701-021-04725-2. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
