

Intraoperative thermal infrared imaging in neurosurgery: machine learning approaches for advanced segmentation of tumors
- PMID: 36715852
- PMCID: PMC10030394
- DOI: 10.1007/s13246-023-01222-x
Intraoperative thermal infrared imaging in neurosurgery: machine learning approaches for advanced segmentation of tumors
Abstract
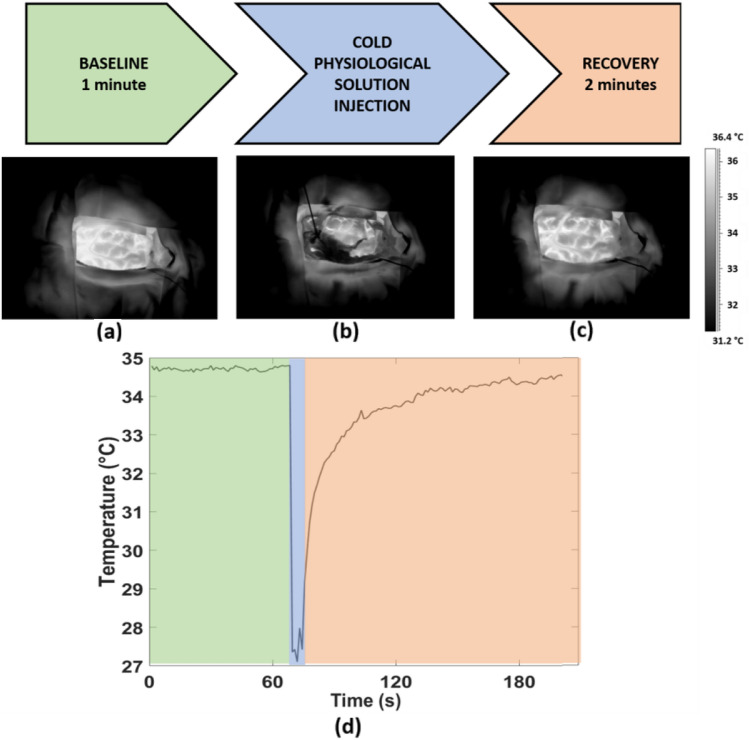
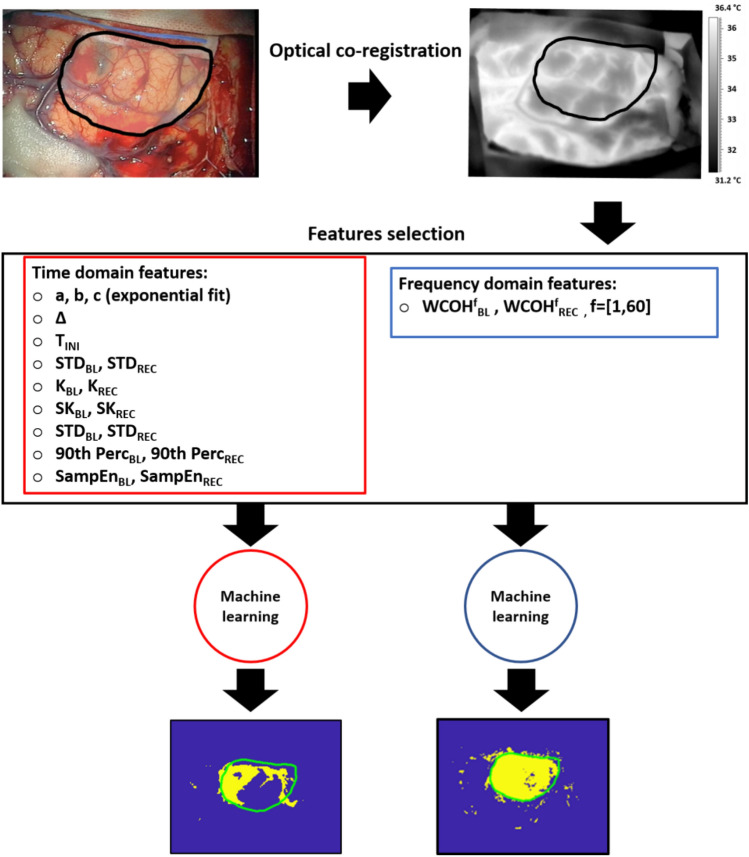
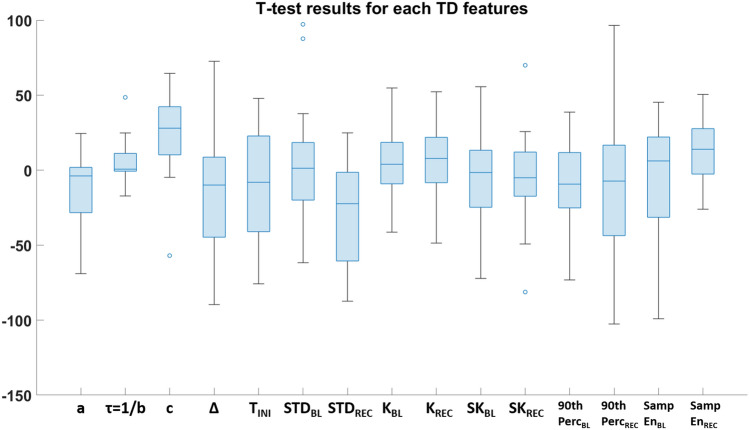
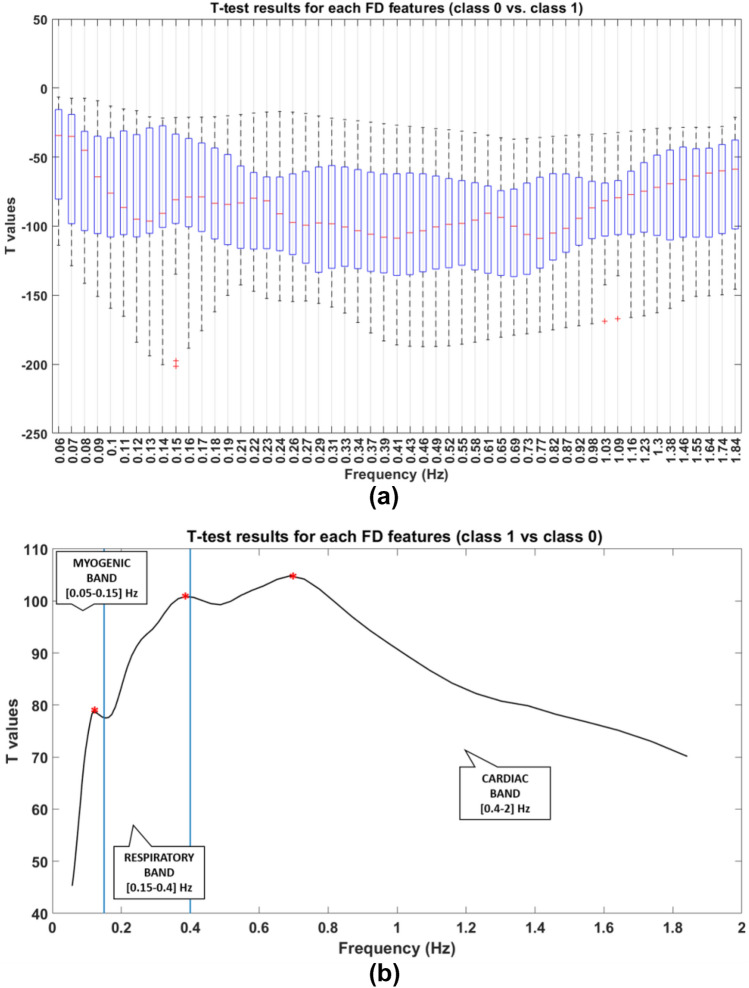
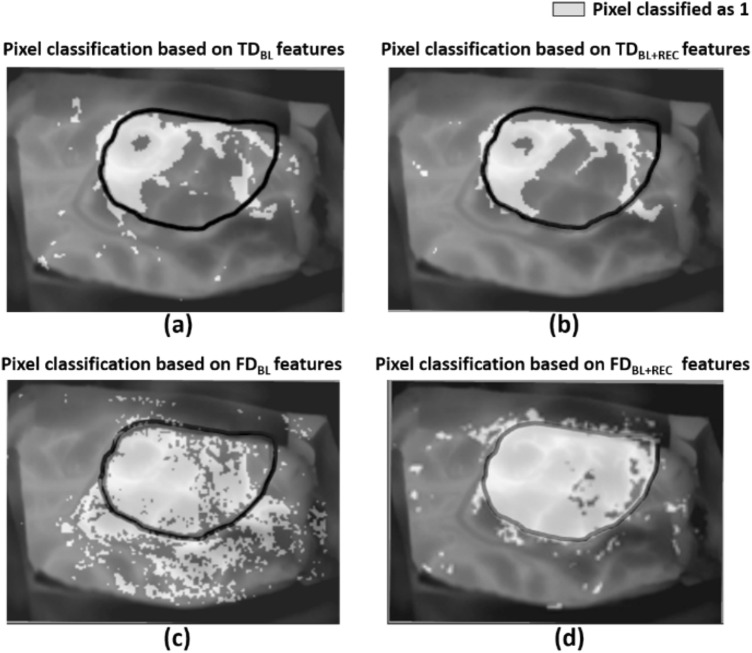
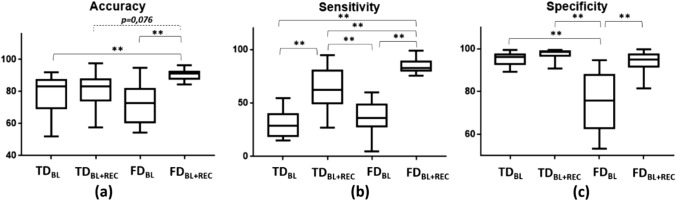
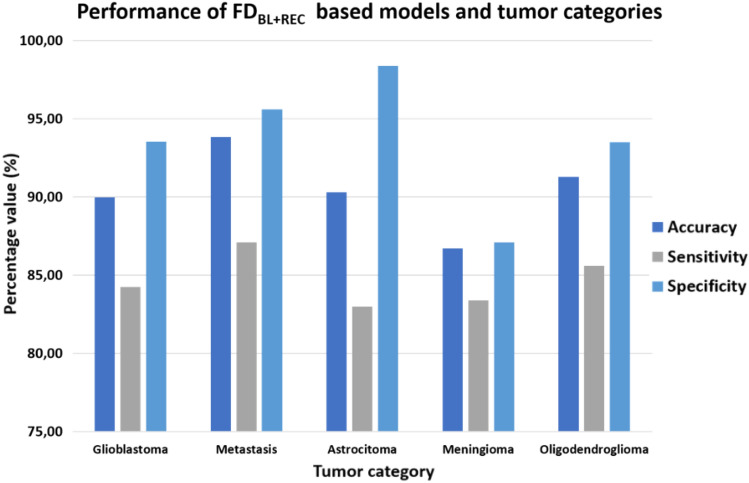
Surgical resection is one of the most relevant practices in neurosurgery. Finding the correct surgical extent of the tumor is a key question and so far several techniques have been employed to assist the neurosurgeon in preserving the maximum amount of healthy tissue. Some of these methods are invasive for patients, not always allowing high precision in the detection of the tumor area. The aim of this study is to overcome these limitations, developing machine learning based models, relying on features obtained from a contactless and non-invasive technique, the thermal infrared (IR) imaging. The thermal IR videos of thirteen patients with heterogeneous tumors were recorded in the intraoperative context. Time (TD)- and frequency (FD)-domain features were extracted and fed different machine learning models. Models relying on FD features have proven to be the best solutions for the optimal detection of the tumor area (Average Accuracy = 90.45%; Average Sensitivity = 84.64%; Average Specificity = 93,74%). The obtained results highlight the possibility to accurately detect the tumor lesion boundary with a completely non-invasive, contactless, and portable technology, revealing thermal IR imaging as a very promising tool for the neurosurgeon.
Keywords: Brain tumor segmentation; Classification; Machine learning; Neurosurgery; Thermal infrared imaging.
© 2023. The Author(s).
Conflict of interest statement
The authors have no relevant financial or non-financial interests to disclose.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical