

B cell response after SARS-CoV-2 mRNA vaccination in people living with HIV
- PMID: 36717688
- PMCID: PMC9886211
- DOI: 10.1038/s43856-023-00245-5
B cell response after SARS-CoV-2 mRNA vaccination in people living with HIV
Abstract
Background: Limited longitudinal data are available on immune response to mRNA SARS-CoV-2 vaccination in people living with HIV (PLWHIV); therefore, new evidence on induction and persistence of spike-specific antibodies and B cells is needed.
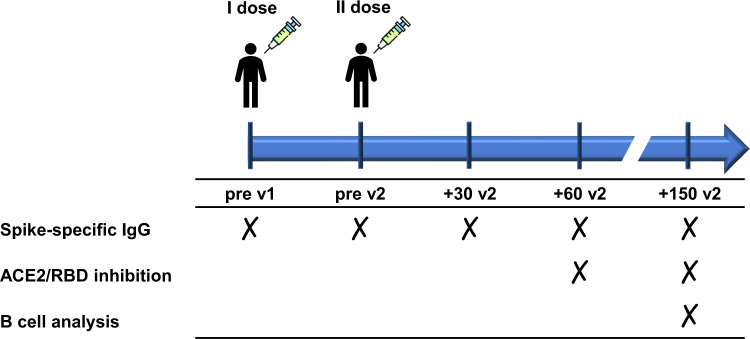
Methods: In this pilot study we investigated the spike-specific humoral and B cell responses up to six months after vaccination with two doses of mRNA vaccines in 84 PLWHIV under antiretroviral therapy compared to 79 healthy controls (HCs).
Results: Spike-specific IgG persisted six months in PLWHIV with no significant differences compared to HCs, even though a significantly lower IgG response was observed in patients with CD4+ T cells < 350/mmc. The frequency of subjects with antibodies capable of inhibiting ACE2/RBD binding was comparable between PLWHIV and HCs a month after the second vaccine dose, then a higher drop was observed in PLWHIV. A comparable percentage of spike-specific memory B cells was observed at month six in PLWHIV and HCs. However, PLWHIV showed a higher frequency of spike-specific IgD- CD27- double-negative memory B cells and a significantly lower rate of IgD- CD27+ Ig-switched memory B cells compared to HCs, suggesting a reduced functionality of the antigen-specific memory B population.
Conclusions: The mRNA vaccination against SARS-CoV-2 elicits humoral and B cell responses quantitatively similar between PLWHIV and HCs, but there are important differences in terms of antibody functionality and phenotypes of memory B cells, reinforcing the notion that tailored vaccination policies should be considered for these patients.
Plain language summary
SARS-CoV-2 vaccination has been demonstrated to protect people from severe COVID-19 and death. This is achieved through the induction of a specific immune response that recognizes and responds to the virus. Limited data are available on the immune response to SARS-CoV-2 vaccination in people living with HIV (PLWHIV). In this study, we evaluated the immune response up to six months after vaccination with two doses of vaccines in PLWHIV being treated with the standard antiretroviral therapy. We show that the immune response observed in PLWHIV is broadly similar to that in healthy subjects but that there are some differences in the cells induced as part of the immune response. We therefore suggest that specific vaccination policies should be considered for these PLWHIV.
© 2023. The Author(s).
Conflict of interest statement
The authors declare the following competing interests. M.F. received speakers’ honoraria, support for travel to meetings, and/or fees for attending advisory boards from Bristol Myers Squibb (BMS), Gilead, Janssen-Cilag, Merck Sharp and Dohme (MSD), and ViiV Healthcare. F.M. received support for travel to meetings from Angelini, she is principal investigator in sponsor study by TLS (Toscana Life Science) and by GSK Vaccine SRL and she is the contact person for a service contract between GSK Vaccine SRL and Department of Medical Biotechnologies, University of Siena, without receiving any personal remuneration. The other authors declare no conflict of interest regarding this study.
Figures


References
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
