

CAR-cell therapy in the era of solid tumor treatment: current challenges and emerging therapeutic advances
- PMID: 36717905
- PMCID: PMC9885707
- DOI: 10.1186/s12943-023-01723-z
CAR-cell therapy in the era of solid tumor treatment: current challenges and emerging therapeutic advances
Abstract
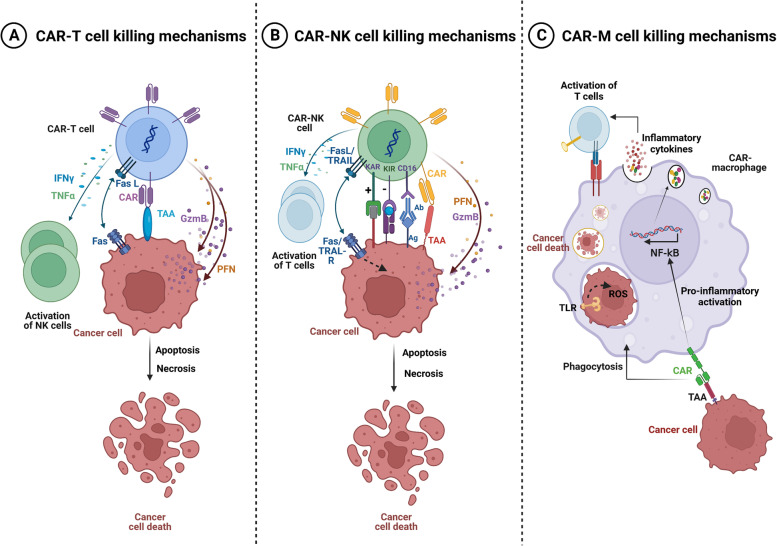
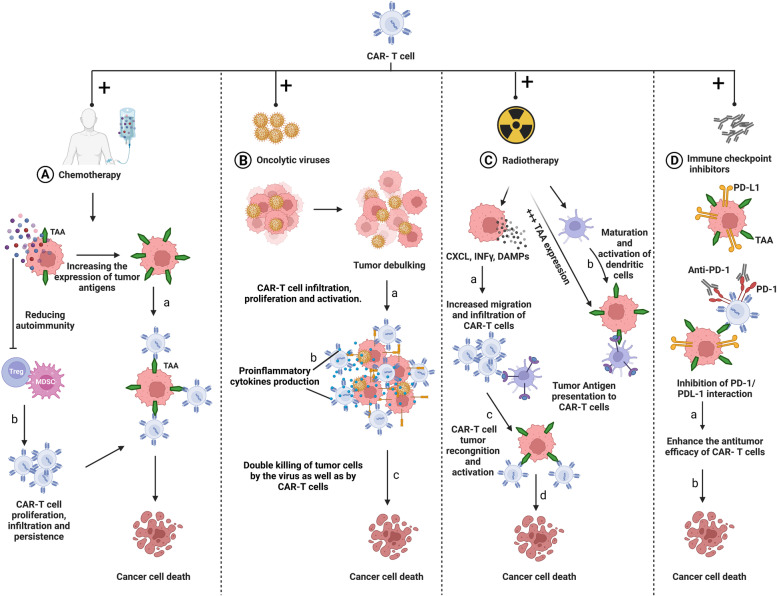
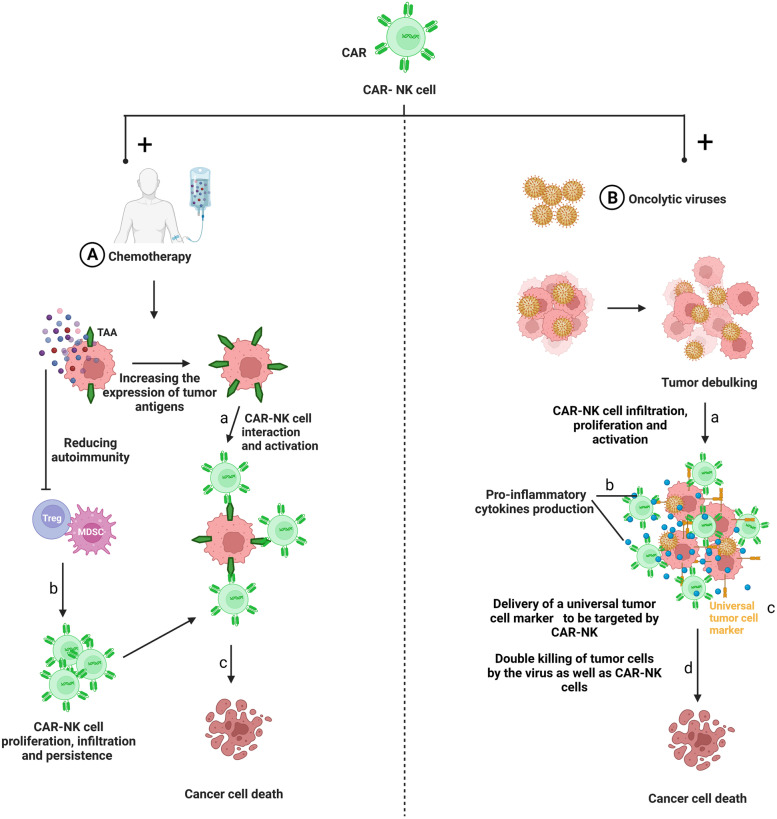
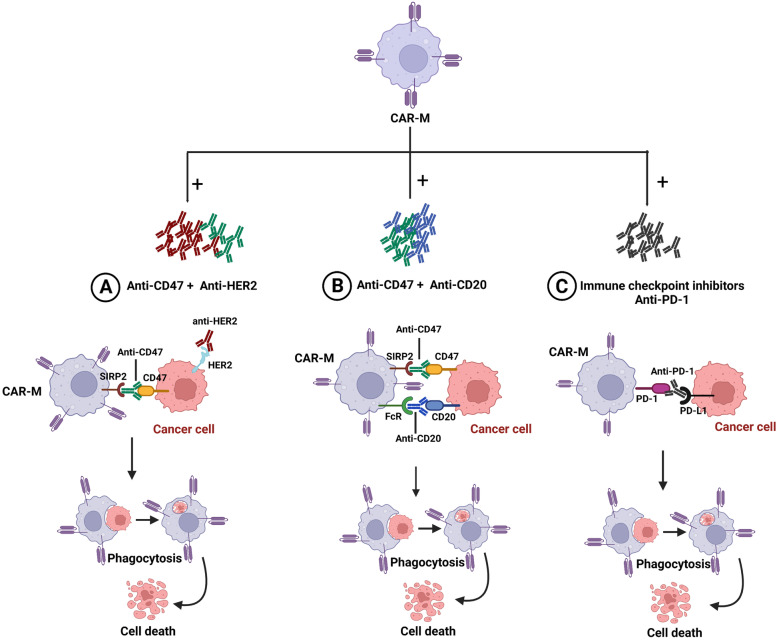
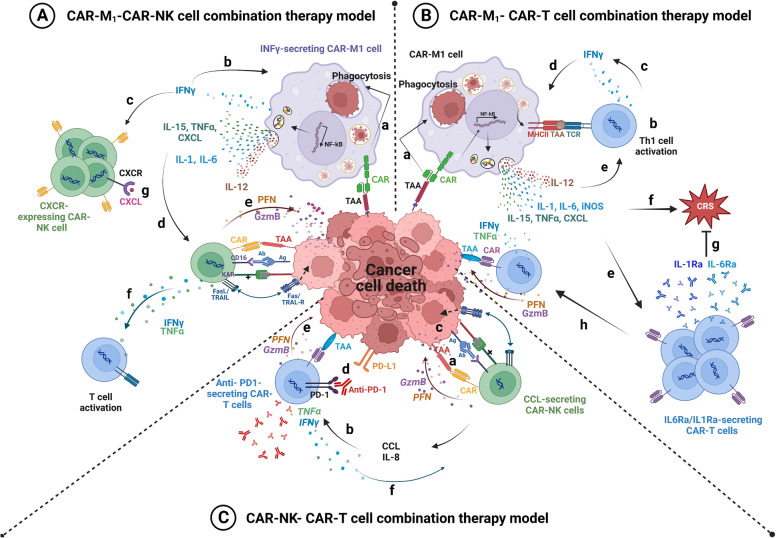
In the last decade, Chimeric Antigen Receptor (CAR)-T cell therapy has emerged as a promising immunotherapeutic approach to fight cancers. This approach consists of genetically engineered immune cells expressing a surface receptor, called CAR, that specifically targets antigens expressed on the surface of tumor cells. In hematological malignancies like leukemias, myeloma, and non-Hodgkin B-cell lymphomas, adoptive CAR-T cell therapy has shown efficacy in treating chemotherapy refractory patients. However, the value of this therapy remains inconclusive in the context of solid tumors and is restrained by several obstacles including limited tumor trafficking and infiltration, the presence of an immunosuppressive tumor microenvironment, as well as adverse events associated with such therapy. Recently, CAR-Natural Killer (CAR-NK) and CAR-macrophages (CAR-M) were introduced as a complement/alternative to CAR-T cell therapy for solid tumors. CAR-NK cells could be a favorable substitute for CAR-T cells since they do not require HLA compatibility and have limited toxicity. Additionally, CAR-NK cells might be generated in large scale from several sources which would suggest them as promising off-the-shelf product. CAR-M immunotherapy with its capabilities of phagocytosis, tumor-antigen presentation, and broad tumor infiltration, is currently being investigated. Here, we discuss the emerging role of CAR-T, CAR-NK, and CAR-M cells in solid tumors. We also highlight the advantages and drawbacks of CAR-NK and CAR-M cells compared to CAR-T cells. Finally, we suggest prospective solutions such as potential combination therapies to enhance the efficacy of CAR-cells immunotherapy.
Keywords: CAR-M; CAR-NK; CAR-T; Cellular immunotherapy; Combined therapies; Solid tumors.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interest.
Figures
References
-
- World Health Organization (WHO) Cancer [https://www.who.int/news-room/fact-sheets/detail/cancer].
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
