

Surgical classification for large macular hole: based on different surgical techniques results: the CLOSE study group
- PMID: 36717928
- PMCID: PMC9885593
- DOI: 10.1186/s40942-022-00439-4
Surgical classification for large macular hole: based on different surgical techniques results: the CLOSE study group
Abstract
Background: The CLOSE study group proposes an updated surgical classification for large macular holes based on a systematic review of new treatments. Recently, many new techniques have been introduced to treat large full-thickness macular holes (FTMH); although the indications are not clear. An updated surgical classification is needed to help surgical decision-making.
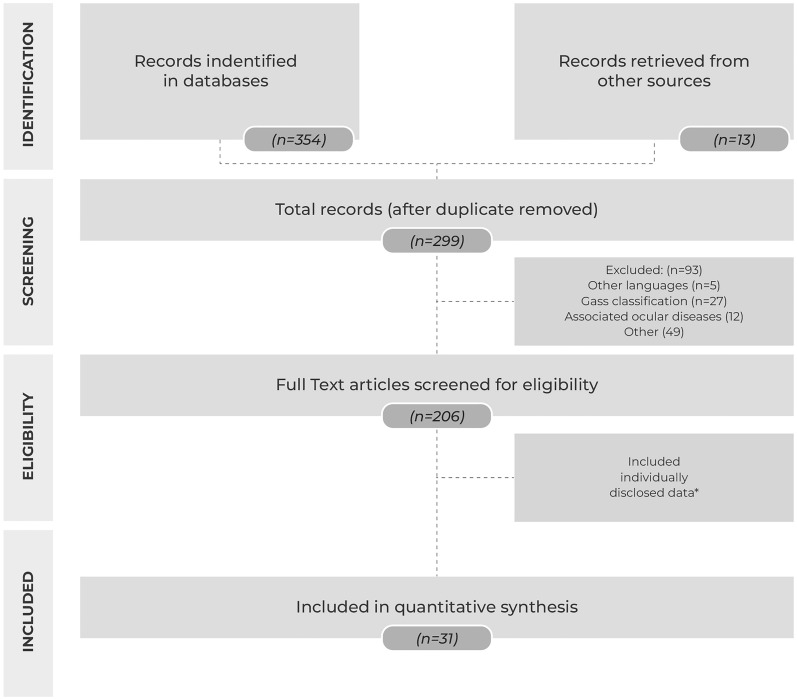
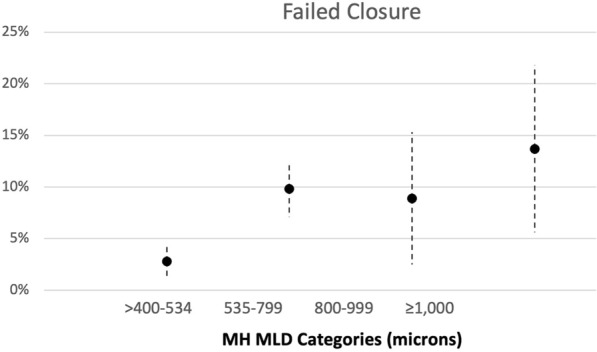
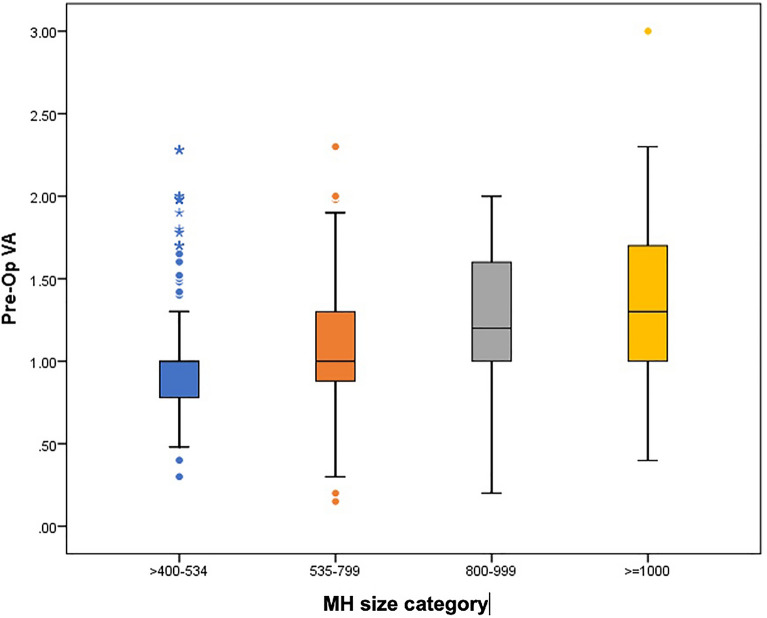
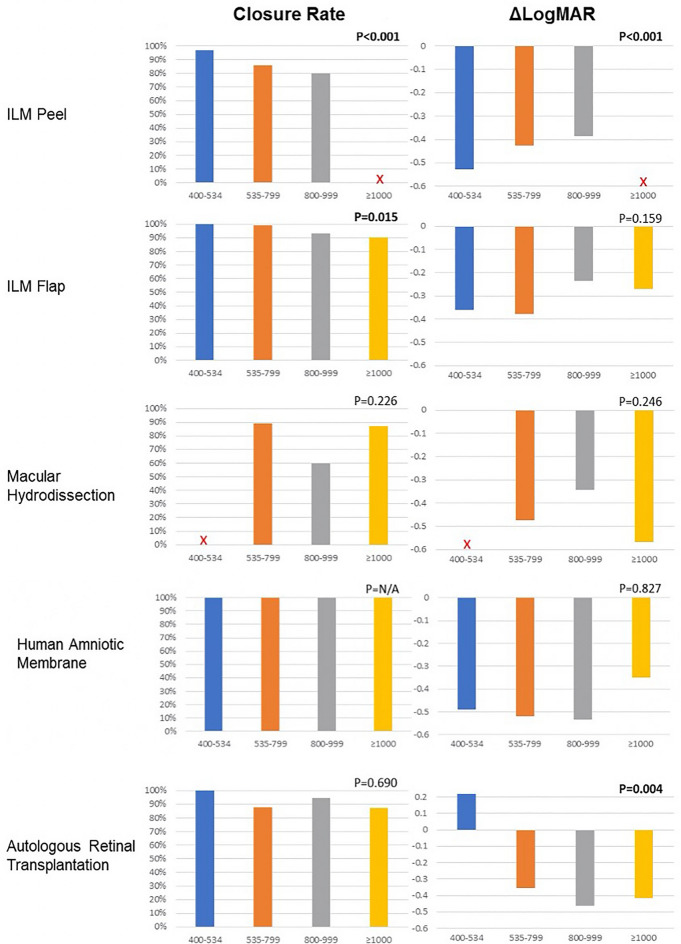
Methods: We gathered published series by the CLOSE Study Group members and from literature search until June 2021. Techniques included: internal limiting membrane peeling (ILM peeling), ILM flaps, macular hydrodissection (macular hydro), human amniotic membrane graft (hAM), and autologous retinal transplantation (ART). Within each technique, chi-square test assessed association between the minimal linear diameter (MLD) (in µm) and closure rate; the postoperative best-corrected visual acuity (BCVA) gains were compared among groups.
Results: Data extraction included 31 published articles: total of 1135 eyes. Eyes were divided into the following groups: ILM peel (n: 683), ILM Flap (n: 233), macular hydrodissection (n: 64), hAM (n: 59), and ART (n: 96). The initial BCVA and size were heterogenous between the groups. ILM peel showed the best results in large FTMH ≤ 535 µm (closure rate 96.8%); adjusted mean BCVA: 0.49 (LogMAR) with a statistical difference among groups. Large FTMH between 535 and 799 µm: ILM flap technique showed better results (closure rate 99.0%); adjusted mean BCVA: 0.67(LogMAR); also with a statistical difference. For large FTMH ≥ 800 µm more invasive techniques are required. Use of hAM, macular hydrodissection and ART showed higher closure rates for this category (100%, 83.3% and 90.5% respectively), and adjusted mean BCVA varied from 0.76 to 0.89. Although there was no statistical difference between those techniques for this group due to the smaller number of cases.
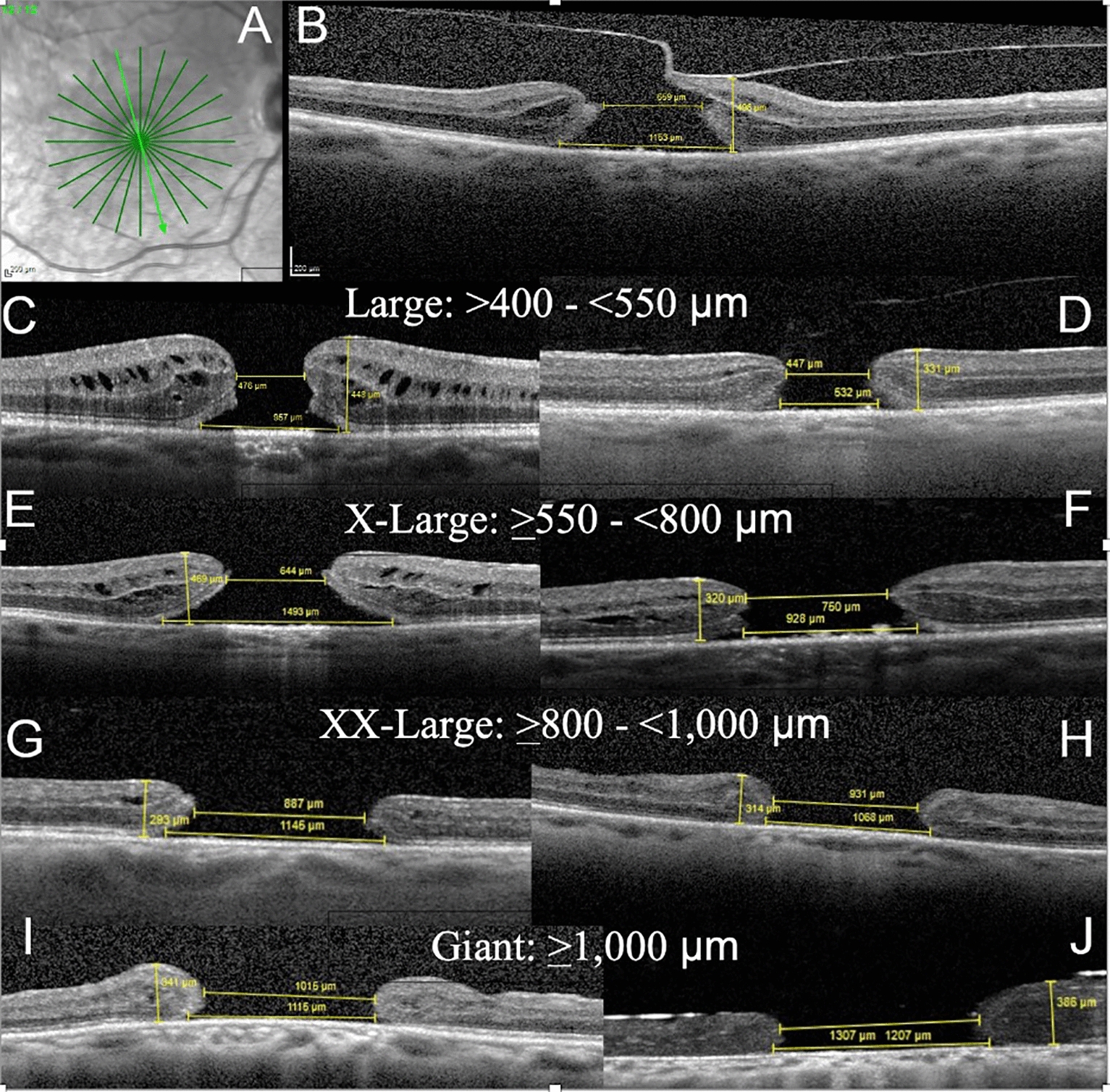
Conclusions: The CLOSE study group demonstrated the potential usefulness of a new surgical classification for large FTMHs and propose OCT biomarkers for use in clinical practice and future research. This new classification demonstrated that Large (400-550 µm) and X-Large (550-800 µm) holes can be treated highly successfully with ILM peel and ILM flap techniques, respectively. Further studies are necessary for the larger FTMHs (XX-Large and Giant), using the CLOSE classification, in order to determine which technique is better suited for each hole size and characteristics.
Keywords: Close study group; Large macular holes; Surgical macular hole classification.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
LinkOut - more resources
Full Text Sources
