

Rationing scarce healthcare capacity: A study of the ventilator allocation guidelines during the COVID-19 pandemic
- PMID: 36718234
- PMCID: PMC9877846
- DOI: 10.1111/poms.13934
Rationing scarce healthcare capacity: A study of the ventilator allocation guidelines during the COVID-19 pandemic
Abstract
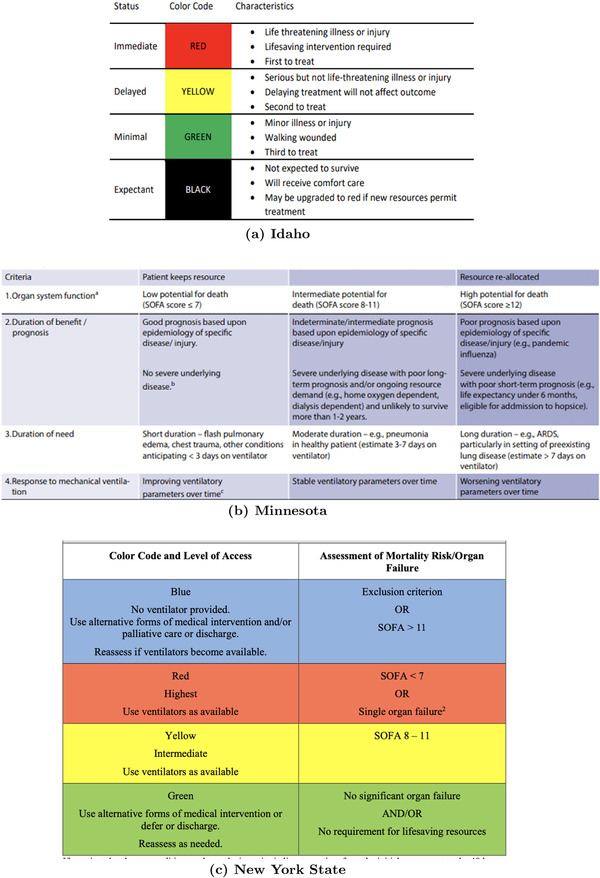
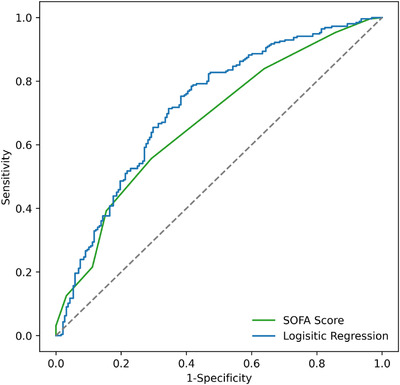
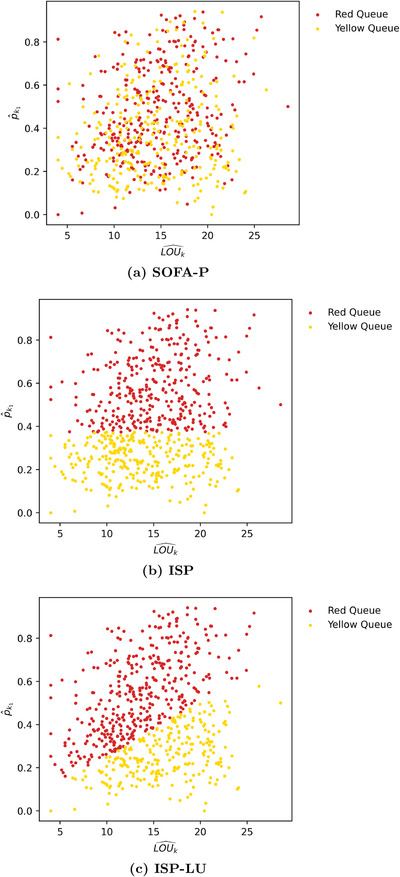
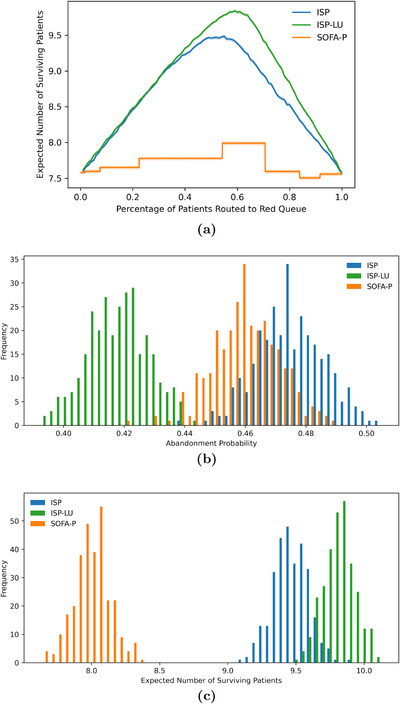
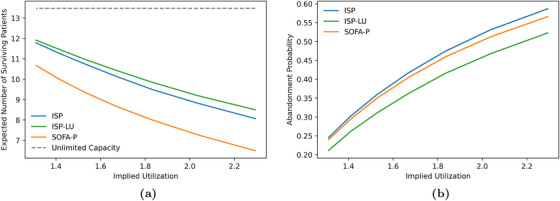
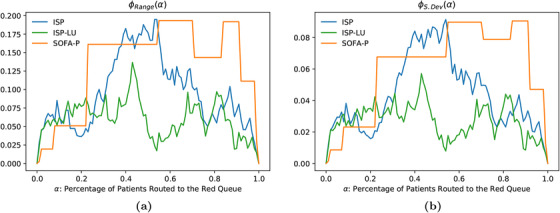
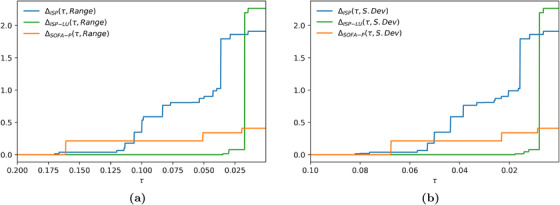
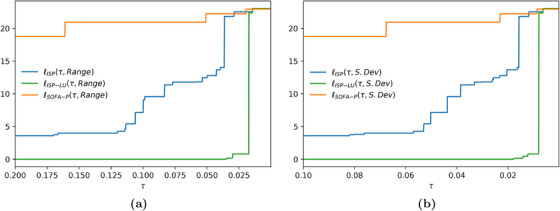
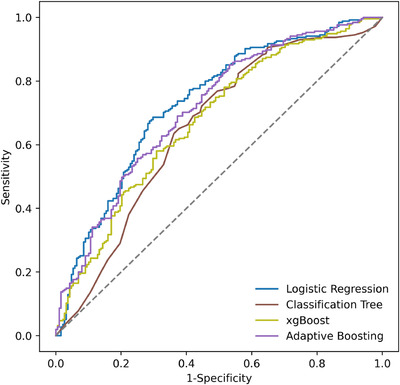
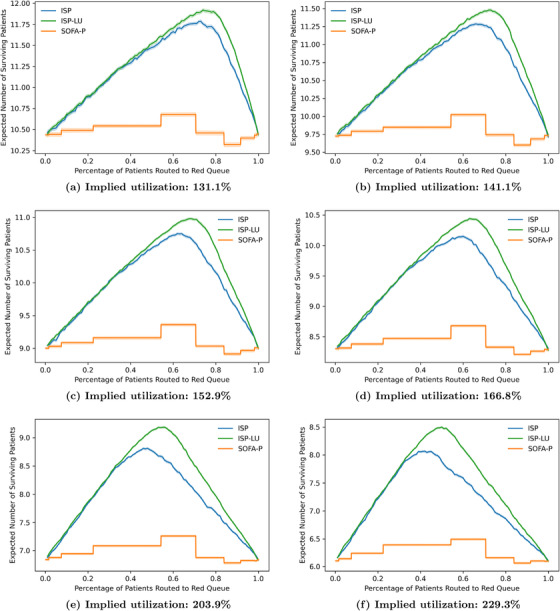
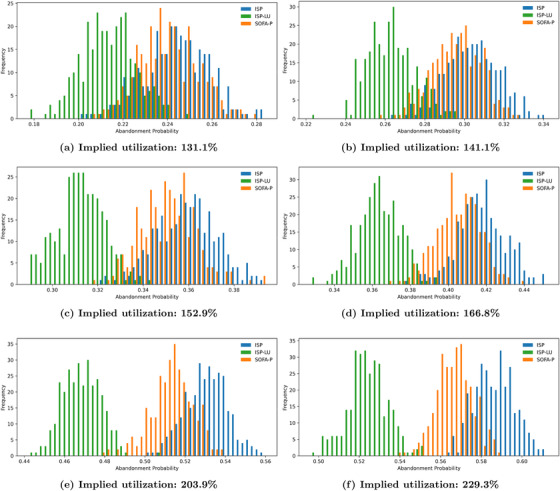
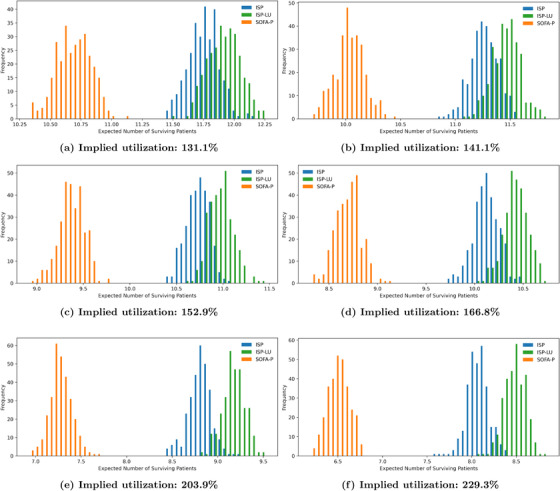
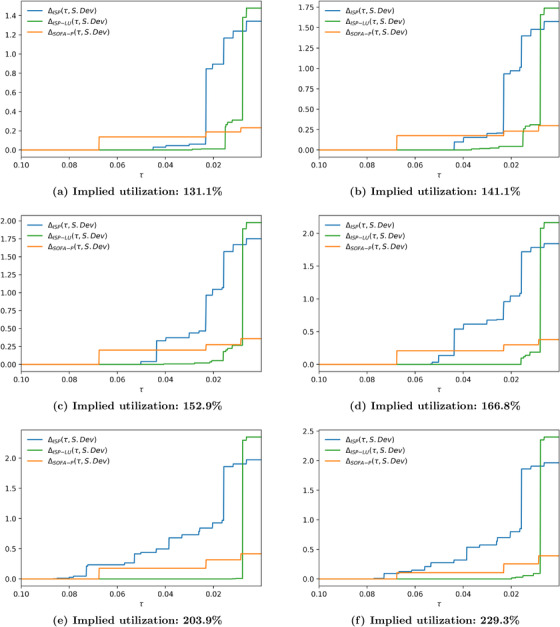
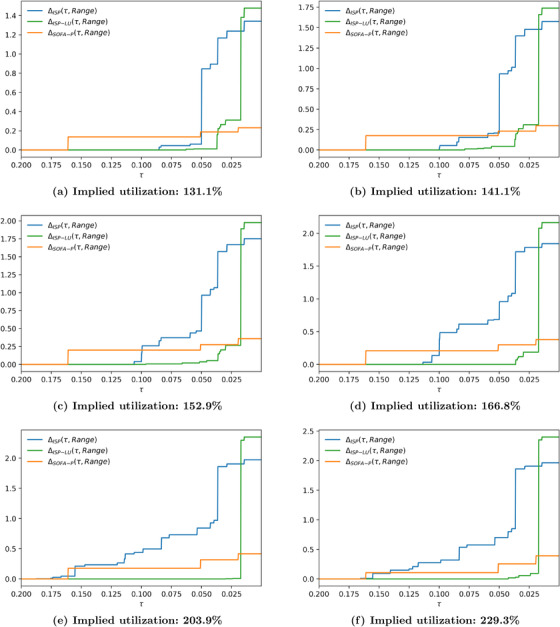
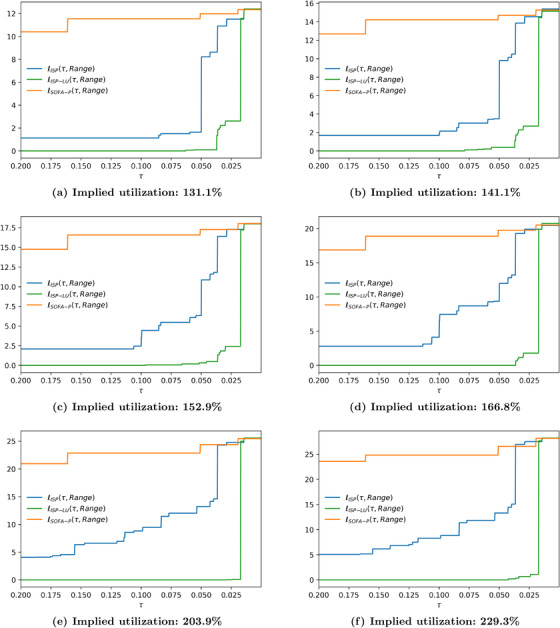
In the United States, even though national guidelines for allocating scarce healthcare resources are lacking, 26 states have specific ventilator allocation guidelines to be invoked in case of a shortage. While several states developed their guidelines in response to the recent COVID-19 pandemic, New York State developed these guidelines in 2015 as "pandemic influenza is a foreseeable threat, one that we cannot ignore." The primary objective of this study is to assess the existing procedures and priority rules in place for allocating/rationing scarce ventilator capacity and propose alternative (and improved) priority schemes. We first build machine learning models using inpatient records of COVID-19 patients admitted to New York-Presbyterian/Columbia University Irving Medical Center and an affiliated community health center to predict survival probabilities as well as ventilator length-of-use. Then, we use the resulting point estimators and their uncertainties as inputs for a multiclass priority queueing model with abandonments to assess three priority schemes: (i) SOFA-P (Sequential Organ Failure Assessment based prioritization), which most closely mimics the existing practice by prioritizing patients with sufficiently low SOFA scores; (ii) ISP (incremental survival probability), which assigns priority based on patient-level survival predictions; and (iii) ISP-LU (incremental survival probability per length-of-use), which takes into account survival predictions and resource use duration. Our findings highlight that our proposed priority scheme, ISP-LU, achieves a demonstrable improvement over the other two alternatives. Specifically, the expected number of survivals increases and death risk while waiting for ventilator use decreases. We also show that ISP-LU is a robust priority scheme whose implementation yields a Pareto-improvement over both SOFA-P and ISP in terms of maximizing saved lives after mechanical ventilation while limiting racial disparity in access to the priority queue.
Keywords: COVID‐19; fairness; machine learning; multiclass queueing with abandonments; priority scheduling; resource allocation; scarce ventilator capacity.
© 2022 Production and Operations Management Society.
Figures

Similar articles
-
Modeling Outcomes Using Sequential Organ Failure Assessment (SOFA) Score-Based Ventilator Triage Guidelines During the COVID-19 Pandemic.Disaster Med Public Health Prep. 2022 Feb 14;17:e128. doi: 10.1017/dmp.2022.37. Disaster Med Public Health Prep. 2022. PMID: 35152936 Free PMC article.
-
Comparison of 2 Triage Scoring Guidelines for Allocation of Mechanical Ventilators.JAMA Netw Open. 2020 Dec 1;3(12):e2029250. doi: 10.1001/jamanetworkopen.2020.29250. JAMA Netw Open. 2020. PMID: 33315112 Free PMC article.
-
Variation in Ventilator Allocation Guidelines by US State During the Coronavirus Disease 2019 Pandemic: A Systematic Review.JAMA Netw Open. 2020 Jun 1;3(6):e2012606. doi: 10.1001/jamanetworkopen.2020.12606. JAMA Netw Open. 2020. PMID: 32558916 Free PMC article.
-
The fairness of ventilator allocation during the COVID-19 pandemic.Bioethics. 2022 Jul;36(6):715-723. doi: 10.1111/bioe.12955. Epub 2021 Sep 18. Bioethics. 2022. PMID: 34536303 Free PMC article.
-
Dialysis resource allocation in critical care: the impact of the COVID-19 pandemic and the promise of big data analytics.Front Nephrol. 2023 Oct 26;3:1266967. doi: 10.3389/fneph.2023.1266967. eCollection 2023. Front Nephrol. 2023. PMID: 37965069 Free PMC article. Review.
Cited by
-
Simulation of New York City's Ventilator Allocation Guideline During the Spring 2020 COVID-19 Surge.JAMA Netw Open. 2023 Oct 2;6(10):e2336736. doi: 10.1001/jamanetworkopen.2023.36736. JAMA Netw Open. 2023. PMID: 37796499 Free PMC article.
References
-
- Ahn, H.‐S. , Silberholz, J. , Song, X. , & Wu, X. (2021). Optimal Covid‐19 containment strategies: Evidence across multiple mathematical models. 10.2139/ssrn.3834668 - DOI
-
- Akan, M. , Alagoz, O. , Ata, B. , Erenay, F. S. , & Said, A. (2012). A broader view of designing the liver allocation system. Operations Research, 60(4), 757–770.
-
- Aleinikoff, T. A. (1991). A case for race‐consciousness. Columbia Law Review, 91(5), 1060–1125.
-
- Almeshari, M. A. , Alobaidi, N. Y. , Al Asmri, M. , Alhuthail, E. , Alshehri, Z. , Alenezi, F. , Sapey, E. , & Parekh, D. (2021). P61 mechanical ventilation utilization in COVID‐19: A systematic review and meta‐analysis. Thorax, 76, A121.1–A121.
-
- Anderson, M. R. , Geleris, J. , Anderson, D. R. , Zucker, J. , Nobel, Y. R. , Freedberg, D. , Small‐Saunders, J. , Rajagopalan, K. N. , Greendyk, R. , Chae, S.‐R. , Natarajan, K. , Roh, D. , Edwin, E. , Gallagher, D. , Podolanczuk, A. , Barr, R. G. , Ferrante, A. W. , & Baldwin, M. R. (2020). Body mass index and risk for intubation or death in SARS‐CoV‐2 infection: A retrospective cohort study. Annals of Internal Medicine, 173(10), 782–790. - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous