

Mechanical Thrombectomy Versus Best Medical Treatment in the Late Time Window in Non-DEFUSE-Non-DAWN Patients: A Multicenter Cohort Study
- PMID: 36718751
- PMCID: PMC10561685
- DOI: 10.1161/STROKEAHA.122.039793
Mechanical Thrombectomy Versus Best Medical Treatment in the Late Time Window in Non-DEFUSE-Non-DAWN Patients: A Multicenter Cohort Study
Abstract
Background: We assessed the efficacy and safety of mechanical thrombectomy (MT) in adult stroke patients with anterior circulation large vessel occlusion presenting in the late time window not fulfilling the DEFUSE-3 (Thrombectomy for Stroke at 6 to 16 Hours With Selection by Perfusion Imaging trial) and DAWN (Thrombectomy 6 to 24 Hours After Stroke With a Mismatch Between Deficit and Infarct trial) inclusion criteria.
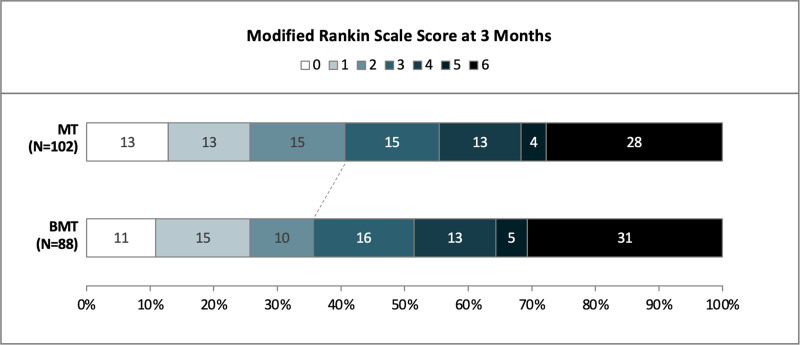
Methods: Cohort study of adults with anterior circulation large vessel occlusion admitted between 6 and 24 hours after last-seen-well at 5 participating Swiss stroke centers between 2014 and 2021. Mismatch was assessed by computer tomography or magnetic resonance imaging perfusion with automated software (RAPID or OLEA). We excluded patients meeting DEFUSE-3 and DAWN inclusion criteria and compared those who underwent MT with those receiving best medical treatment alone by inverse probability of treatment weighting using the propensity score. The primary efficacy end point was a favorable functional outcome at 90 days, defined as a modified Rankin Scale score shift toward lower categories. The primary safety end point was symptomatic intracranial hemorrhage within 7 days of stroke onset; the secondary was all-cause mortality within 90 days.
Results: Among 278 patients with anterior circulation large vessel occlusion presenting in the late time window, 190 (68%) did not meet the DEFUSE-3 and DAWN inclusion criteria and thus were included in the analyses. Of those, 102 (54%) received MT. In the inverse probability of treatment weighting analysis, patients in the MT group had higher odds of favorable outcomes compared with the best medical treatment alone group (modified Rankin Scale shift: acOR, 1.46 [1.02-2.10]; P=0.04) and lower odds of all-cause mortality within 90 days (aOR, 0.59 [0.37-0.93]; P=0.02). There were no significant differences in symptomatic intracranial hemorrhage (MT versus best medical treatment alone: 5% versus 2%, P=0.63).
Conclusions: Two out of 3 patients with anterior circulation large vessel occlusion presenting in the late time window did not meet the DEFUSE-3 and DAWN inclusion criteria. In these patients, MT was associated with higher odds of favorable functional outcomes without increased rates of symptomatic intracranial hemorrhage. These findings support the enrollment of patients into ongoing randomized trials on MT in the late window with more permissive inclusion criteria.
Keywords: acute stroke; patient selection; reperfusion; thrombectomy.
Conflict of interest statement
MK received speaker honoraria from Medtronic. LHB received personal fees from Claret Medical and InnovHeart. UF reports research grants from Medtronic for the SWIFT DIRECT trial (Solitaire With the Intention for Thrombectomy Plus Intravenous t-PA Versus DIRECT Solitaire Stent-Retriever Thrombectomy in Acute Anterior Circulation Stroke) and BEYOND SWIFT registry (Registry for Evaluating Outcome of Acute Ischemic Stroke Patients Treated With Mechanical Thrombectomy); consulting fees from Medtronic, Stryker and CSL Behring (fees paid to institution); membership of a Data Safety Monitoring Board for the IN EXTREMIS trial (Large Stroke Therapy Evaluation) and TITAN trial (Thrombectomy in Tandem Occlusion). GMDM received speaker honoraria from Medtronic. The other authors report no conflicts of interest.
Figures

Comment in
-
Mechanical Thrombectomy in Late-Time Windows: Time to Treat More Patients.Stroke. 2023 Mar;54(3):731-732. doi: 10.1161/STROKEAHA.122.041420. Epub 2023 Jan 31. Stroke. 2023. PMID: 36718750 No abstract available.
References
-
- Ribo M, Molina CA, Cobo E, Cerdà N, Tomasello A, Quesada H, De Miquel MA, Millan M, Castaño C, Urra X, et al. . Association between time to reperfusion and outcome is primarily driven by the time from imaging to reperfusion. Stroke. 2016;47:999–1004. doi: 10.1161/strokeaha.115.011721 - PubMed
-
- Berkhemer OA, Fransen PS, Beumer D, van den Berg LA, Lingsma HF, Yoo AJ, Schonewille WJ, Vos JA, Nederkoorn PJ, Wermer MJ, et al. . A randomized trial of intraarterial treatment for acute ischemic stroke. N Engl J Med. 2015;372:11–20. doi: 10.1056/NEJMoa1411587 - PubMed
-
- Saver JL, Goyal M, Bonafe A, Diener HC, Levy EI, Pereira VM, Albers GW, Cognard C, Cohen DJ, Hacke W, et al. . Stent-retriever thrombectomy after intravenous t-PA vs. t-PA alone in stroke. N Engl J Med. 2015;372:2285–2295. doi: 10.1056/nejmoa1415061 - PubMed
-
- Campbell BC, Mitchell PJ, Kleinig TJ, Dewey HM, Churilov L, Yassi N, Yan B, Dowling RJ, Parsons MW, Oxley TJ, et al. . Endovascular therapy for ischemic stroke with perfusion-imaging selection. N Engl J Med. 2015;372:1009–1018. doi: 10.1056/nejmoa1414792 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
