

Tolvaptan for Children and Adolescents with Autosomal Dominant Polycystic Kidney Disease: Randomized Controlled Trial
- PMID: 36719158
- PMCID: PMC10101612
- DOI: 10.2215/CJN.0000000000000022
Tolvaptan for Children and Adolescents with Autosomal Dominant Polycystic Kidney Disease: Randomized Controlled Trial
Abstract
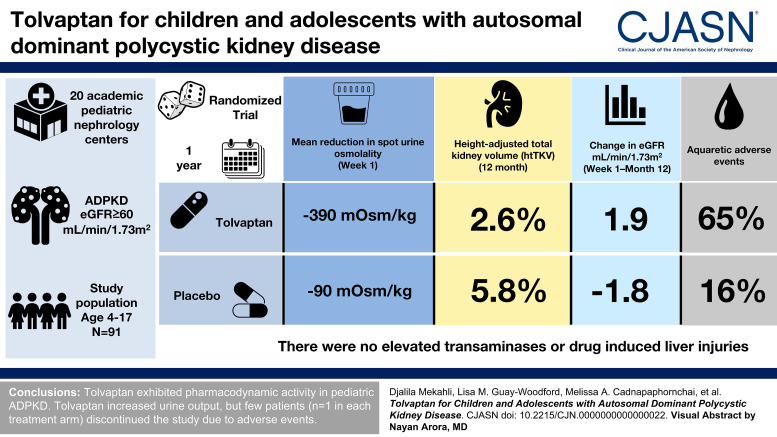
Background: Tolvaptan slows expansion of kidney volume and kidney function decline in adults with autosomal dominant polycystic kidney disease (ADPKD). Progression during childhood could be treated before irreversible kidney damage occurs, but trial data are lacking. We evaluated the safety and efficacy of tolvaptan in children/adolescents with ADPKD.
Methods: This was the 1-year, randomized, double-blind, portion of a phase 3b, two-part trial being conducted at 20 academic pediatric nephrology centers. Key eligibility criteria were ADPKD and eGFR ≥60 ml/min per 1.73 m2. Participants aged 12-17 years were the target group (group 1, enrollment goal n≥60); participants aged 4-11 years could additionally enroll (group 2, anticipated enrollment approximately 40). Treatments were tolvaptan or placebo titrated by body weight and tolerability. Coprimary end points, change from baseline in spot urine osmolality and specific gravity at week 1, assessed inhibition of antidiuretic hormone activity. The key secondary end point was change in height-adjusted total kidney volume (htTKV) to month 12 in group 1. Additional end points were safety/tolerability and quality of life. Statistical comparisons were exploratory and post hoc.
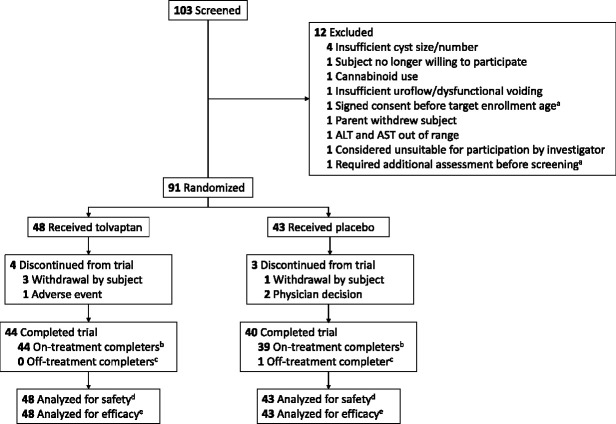
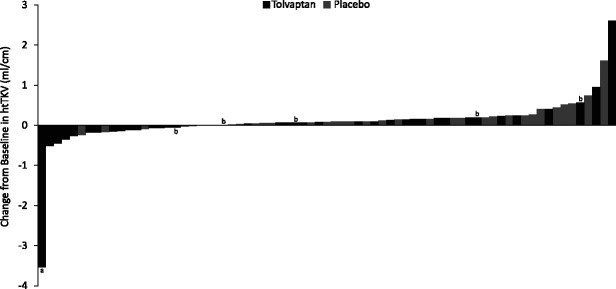
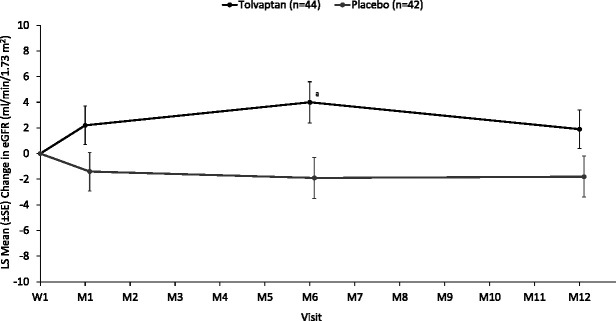
Results: Among the 91 randomized (group 1, n=66; group 2, n=25), least squares (LS) mean reduction (±SEM) in spot urine osmolality at week 1 was greater with tolvaptan (-390 [28] mOsm/kg) than placebo (-90 [29] mOsm/kg; P<0.001), as was LS mean reduction in specific gravity (-0.009 [0.001] versus -0.002 [0.001]; P<0.001). In group 1, the 12-month htTKV increase was 2.6% with tolvaptan and 5.8% with placebo (P>0.05). For tolvaptan and placebo, respectively, 65% and 16% of subjects experienced aquaretic adverse events, and 2% and 0% experienced hypernatremia. There were no elevated transaminases or drug-induced liver injuries. Four participants discontinued tolvaptan, and three discontinued placebo. Quality-of-life assessments remained stable.
Conclusions: Tolvaptan exhibited pharmacodynamic activity in pediatric ADPKD. Aquaretic effects were manageable, with few discontinuations.
Clinical trial registry name and registration number: Safety, Pharmacokinetics, Tolerability and Efficacy of Tolvaptan in Children and Adolescents With ADPKD (Autosomal Dominant Polycystic Kidney Disease) NCT02964273.
Copyright © 2023 by the American Society of Nephrology.
Conflict of interest statement
M.A. Cadnapaphornchai reports consultancy agreements with Otsuka Pharmaceutical, honoraria from Otsuka, and an advisory or leadership role for Otsuka Tolvaptan pediatric steering committee. A. Dandurand reports employment with Cerevel Therapeutics and was an employee of Otsuka at the time of the study. A. Dandurand's spouse reports employment with Cerberus Sentinel. L.A. Greenbaum reports consultancy agreements with Advicenne, Alexion, Arrowhead Pharmaceuticals, Aurinia, Cara Therapeutics, Handok, Natera, Novartis, Otsuka, and Roche; research funding from AbbVie, Advicenne, Alexion, Apellis, Aurinia, Reata Pharmaceuticals, Roche, and Vertex; honoraria from Alexion and Otsuka; advisory or leadership role for Alexion; and DSMB payments for Akebia, Alnylam, Reata, Relypsa, Travere, and UCSD. L.M. Guay-Woodford serves a consultant for and receives honoraria from Natera, Inc. and Otsuka Pharmaceutical. M. Litwin reports consultancy agreements with Alnylam, Bayer, Otsuka, and Travere; honoraria from Alnylam, Bayer, Otsuka, and Travere; and advisory or leadership roles for Bayer and Otsuka. D. Mekahli reports consultancy for Otsuka Pharmaceuticals and Reata as a representative of the University Hospital of Leuven and the KU Leuven University; educational grants from Otsuka Pharmaceuticals and Galapagos paid to the University Hospital of Leuven—all outside the submitted work; serves on an advisory board of Galapagos, Otsuka Pharmaceuticals, Reata, and Sanofi Genzyme as a representative of the University Hospital of Leuven and KU Leuven; is a member of the European Reference Network for Rare Kidney Diseases (ERKNet); and is supported by the clinical research fund of UZ Leuven (Belgium) and the Research Foundation Flanders (FWO; G0C8920N; 1804123N). F. Schaefer reports consultancy agreements with Akebia, Alexion, Alnylam, Amgen, Astellas, AstraZeneca, Bayer, Boehringer Ingelheim, Fresenius Medical Care, GSK, Otsuka, Purespring, Relypsa, and Roche; research funding from Fresenius Medical Care; honoraria from Amgen, Kyowa Kirin, Otsuka, and Roche; textbook royalties from Springer; Scientific Advisory Board activities for Alexion and Otsuka; and is a member of ERKNet. T. Seeman reports consultancy agreements with Otsuka Pharmaceutical. L. Shi, S.E. Shoaf, and K. Sikes are employees of Otsuka Pharmaceutical.
Figures
Comment in
-
Tolvaptan for Autosomal Dominant Polycystic Kidney Disease in Children: Why, Who, and When?Clin J Am Soc Nephrol. 2023 Jan 1;18(1):11-13. doi: 10.2215/CJN.0000000000000028. Clin J Am Soc Nephrol. 2023. PMID: 36719155 Free PMC article. No abstract available.
References
-
- Seeman T Dusek J Vondrák K, et al. Renal concentrating capacity is linked to blood pressure in children with autosomal dominant polycystic kidney disease. Physiol Res. 2004;53:629-634. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
