

Ablative Margins of Colorectal Liver Metastases Using Deformable CT Image Registration and Autosegmentation
- PMID: 36719291
- PMCID: PMC10102669
- DOI: 10.1148/radiol.221373
Ablative Margins of Colorectal Liver Metastases Using Deformable CT Image Registration and Autosegmentation
Abstract
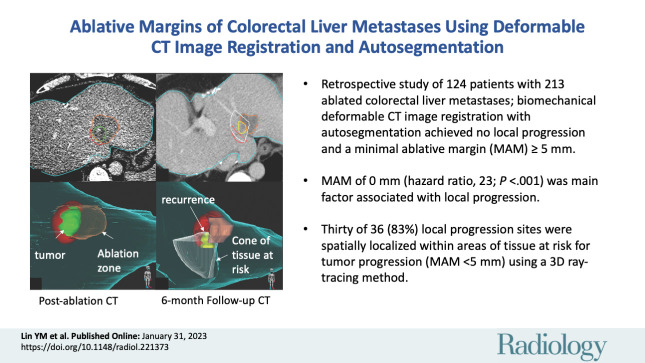
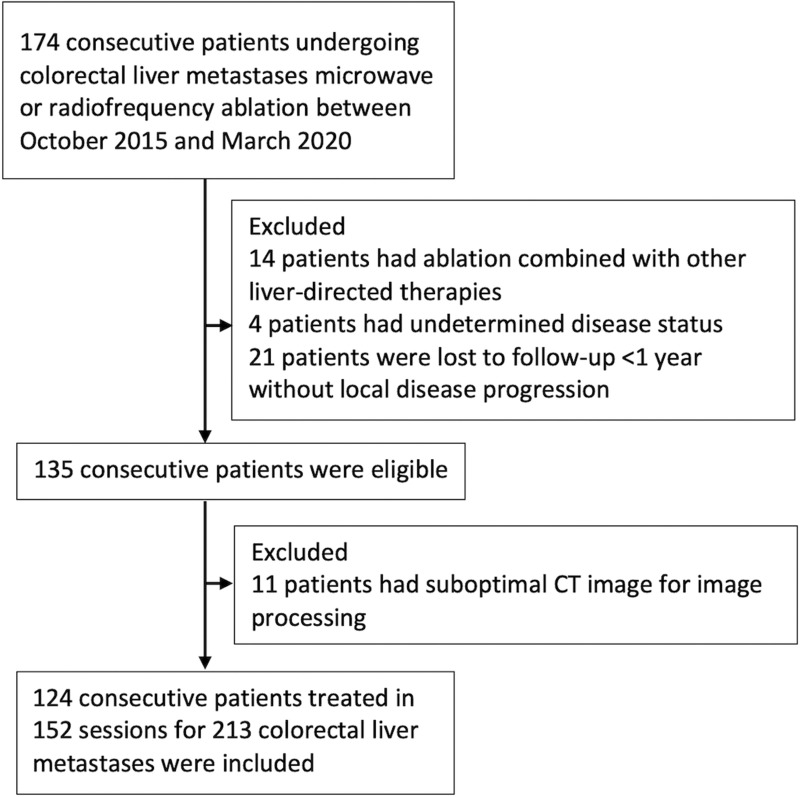
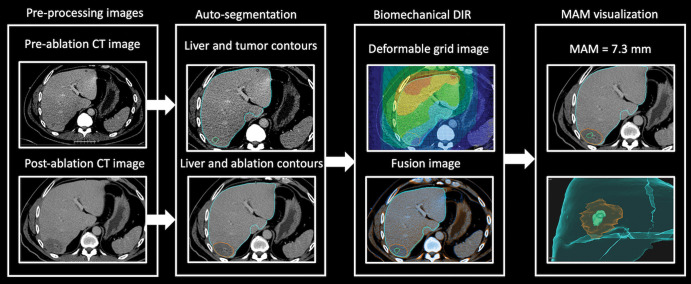
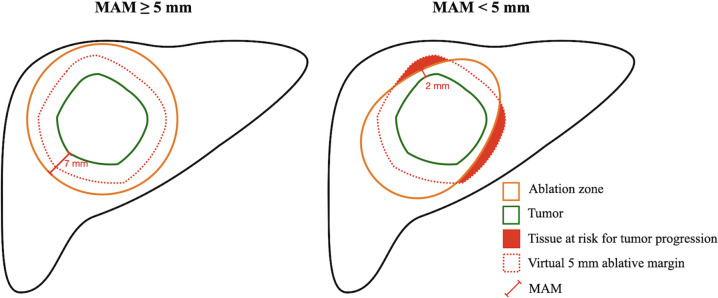
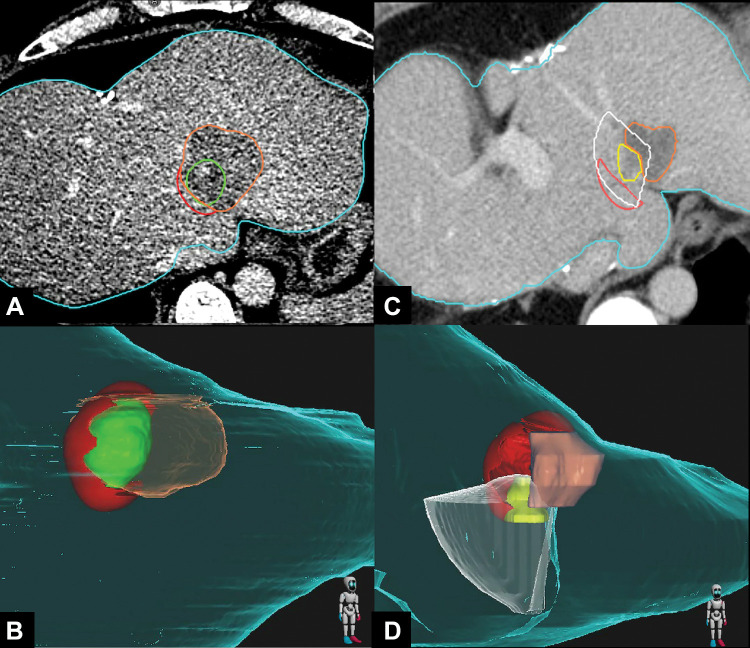
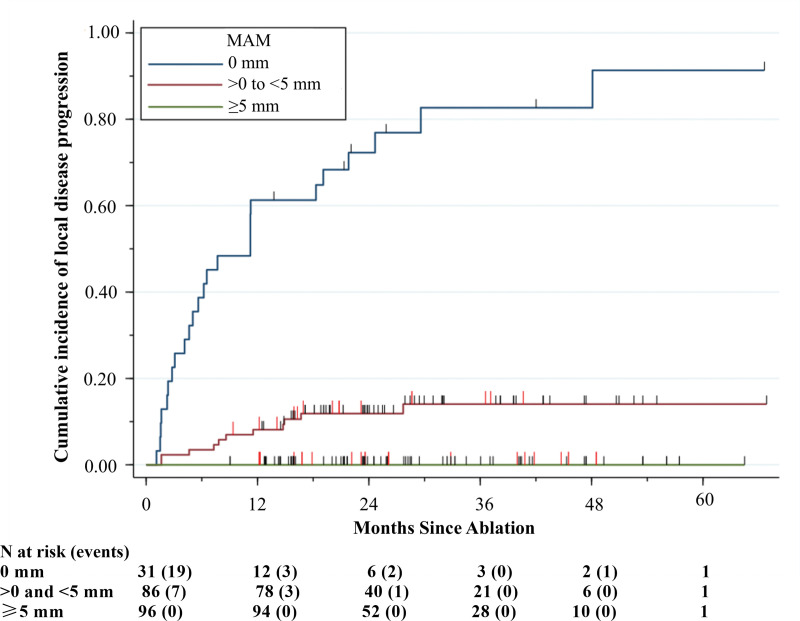
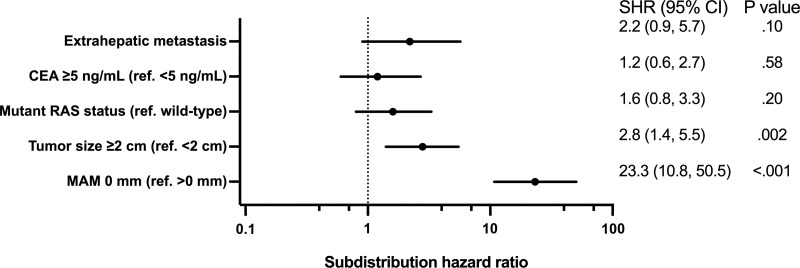
Background Confirming ablation completeness with sufficient ablative margin is critical for local tumor control following colorectal liver metastasis (CLM) ablation. An image-based confirmation method considering patient- and ablation-related biomechanical deformation is an unmet need. Purpose To evaluate a biomechanical deformable image registration (DIR) method for three-dimensional (3D) minimal ablative margin (MAM) quantification and the association with local disease progression following CT-guided CLM ablation. Materials and Methods This single-institution retrospective study included patients with CLM treated with CT-guided microwave or radiofrequency ablation from October 2015 to March 2020. A biomechanical DIR method with AI-based autosegmentation of liver, tumors, and ablation zones on CT images was applied for MAM quantification retrospectively. The per-tumor incidence of local disease progression was defined as residual tumor or local tumor progression. Factors associated with local disease progression were evaluated using the multivariable Fine-Gray subdistribution hazard model. Local disease progression sites were spatially localized with the tissue at risk for tumor progression (<5 mm) using a 3D ray-tracing method. Results Overall, 213 ablated CLMs (mean diameter, 1.4 cm) in 124 consecutive patients (mean age, 57 years ± 12 [SD]; 69 women) were evaluated, with a median follow-up interval of 25.8 months. In ablated CLMs, an MAM of 0 mm was depicted in 14.6% (31 of 213), from greater than 0 to less than 5 mm in 40.4% (86 of 213), and greater than or equal to 5 mm in 45.1% (96 of 213). The 2-year cumulative incidence of local disease progression was 72% for 0 mm and 12% for greater than 0 to less than 5 mm. No local disease progression was observed for an MAM greater than or equal to 5 mm. Among 117 tumors with an MAM less than 5 mm, 36 had local disease progression and 30 were spatially localized within the tissue at risk for tumor progression. On multivariable analysis, an MAM of 0 mm (subdistribution hazard ratio, 23.3; 95% CI: 10.8, 50.5; P < .001) was independently associated with local disease progression. Conclusion Biomechanical deformable image registration and autosegmentation on CT images enabled identification and spatial localization of colorectal liver metastases at risk for local disease progression following ablation, with a minimal ablative margin greater than or equal to 5 mm as the optimal end point. © RSNA, 2023 Supplemental material is available for this article. See also the editorial by Sofocleous in this issue.
Conflict of interest statement
Figures
Comment in
-
Automated Segmentation of CT-guided Ablation Margins in Colorectal Liver Metastases: How We Move Forward to a Standardization of Ablation Zone Assessment.Radiology. 2023 Apr;307(2):e223276. doi: 10.1148/radiol.223276. Epub 2023 Jan 31. Radiology. 2023. PMID: 36719295 Free PMC article. No abstract available.
References
-
- National Comprehensive Cancer Network . Colon Cancer (Version 1.2022) . https://www.nccn.org/professionals/physician_gls/pdf/colon.pdf. Accessed August 17, 2022 .
-
- Otto G , Düber C , Hoppe-Lotichius M , König J , Heise M , Pitton MB . Radiofrequency ablation as first-line treatment in patients with early colorectal liver metastases amenable to surgery . Ann Surg 2010. ; 251 ( 5 ): 796 – 803 . - PubMed
-
- Mulier S , Ni Y , Jamart J , Michel L , Marchal G , Ruers T . Radiofrequency ablation versus resection for resectable colorectal liver metastases: time for a randomized trial? Ann Surg Oncol 2008. ; 15 ( 1 ): 144 – 157 . - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
