

Cervical spine injury: clinical and medico-legal overview
- PMID: 36719553
- PMCID: PMC9931800
- DOI: 10.1007/s11547-022-01578-2
Cervical spine injury: clinical and medico-legal overview
Abstract
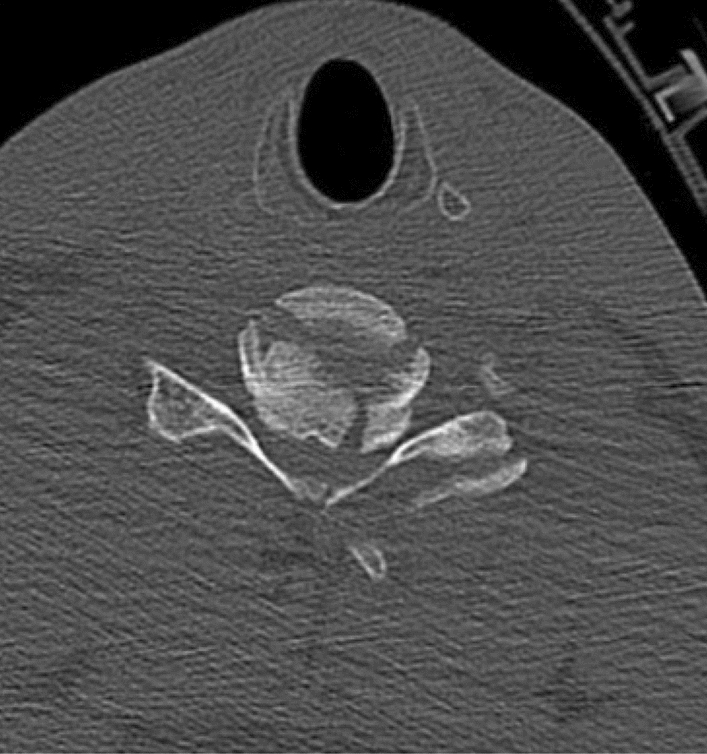
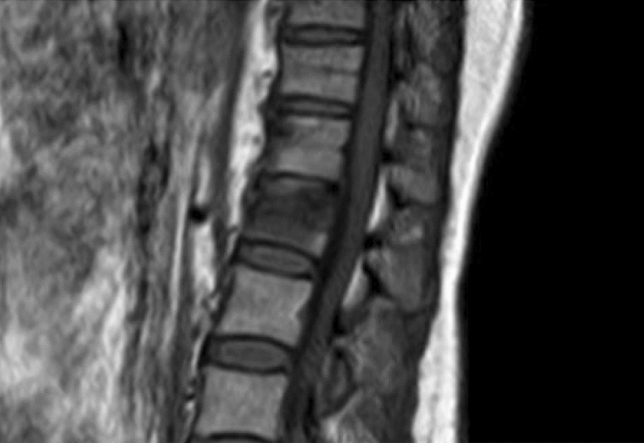
Spinal trauma is an important cause of disability worldwide. Injury to the cervical spine (CS) occurs frequently after major trauma. 5-10% of patients with blunt trauma have a cervical spine injury. The cervical spine accounts for ~ 50% of all spinal injuries. Determination of CS stability is a common challenge in the acute care setting of patients with trauma. Several issues, indeed, are of particular concern: who needs CS imaging; what imaging should be obtained; when should computed tomography (CT), magnetic resonance imaging (MRI), or flexion/extension (F/E) radiographs be obtained; and how is significant ligamentous injury excluded in the comatose patient. CT and MRI both have roles to play. This article aims to present the different imaging to frame techniques to be used with greater precision in the acute event also for the purpose of planning the next therapeutic process. An overview of the applicability of the same methods in forensic pathology is also provided highlighting possible future biomarker to ease in diagnosis of acute TBI.
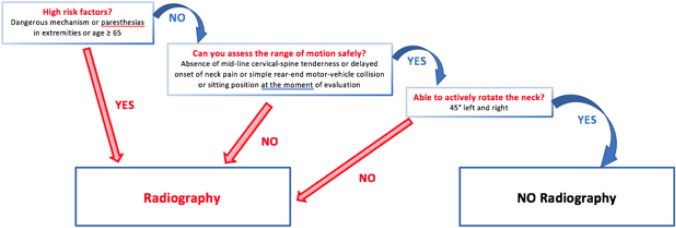
Keywords: Canadian C-spine rule; Cervical spine imaging; Cervical spine injury; NEXUS criteria; Post-mortem imaging.
© 2023. The Author(s).
Conflict of interest statement
The authors have not disclosed any competing interests.
Figures



References
-
- Como JJ, Diaz JJ, Dunham CM, et al. Practice management guidelines for identification of cervical spine injuries following trauma: update from the eastern association for the surgery of trauma practice management guidelines committee. J Trauma. 2009;67:651–659. doi: 10.1097/TA.0B013E3181AE583B. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
