

Automated image fusion during endovascular aneurysm repair: a feasibility and accuracy study
- PMID: 36719561
- PMCID: PMC10363050
- DOI: 10.1007/s11548-023-02832-2
Automated image fusion during endovascular aneurysm repair: a feasibility and accuracy study
Abstract
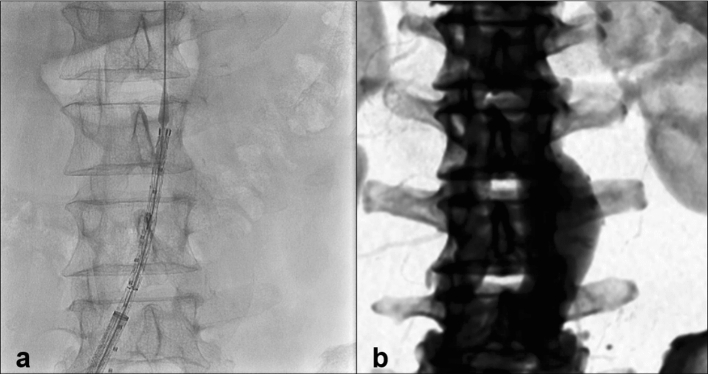
Purpose: Image fusion merges preoperative computed tomography angiography (CTA) with live fluoroscopy during endovascular procedures to function as an overlay 3D roadmap. However, in most current systems, the registration between imaging modalities is performed manually by vertebral column matching which can be subjective, inaccurate and time consuming depending on experience. Our objective was to evaluate feasibility and accuracy of image-based automated 2D-3D image fusion between preoperative CTA and intraoperative fluoroscopy based on vertebral column matching.
Methods: A single-center study with offline procedure data was conducted in 10 consecutive patients which had endovascular aortic repair in which we evaluated unreleased automated fusion software provided by Philips (Best, the Netherlands). Fluoroscopy and digital subtraction angiography images were collected after the procedures and the vertebral column was fused fully automatically. Primary endpoints were feasibility and accuracy of bone alignment (mm). Secondary endpoint was vascular alignment (mm) between the lowest renal artery orifices. Clinical non-inferiority was defined at a mismatch of < 1 mm.
Results: In total, 87 automated measurements and 40 manual measurements were performed on vertebrae T12-L5 in all 10 patients. Manual correction was needed in 3 of the 10 patients due to incomplete visibility of the vertebral edges in the fluoroscopy image. Median difference between automated fusion and manual fusion was 0.1 mm for bone alignment (p = 0.94). The vascular alignment was 4.9 mm (0.7-17.5 mm) for manual and 5.5 mm (1.0-14.0 mm) for automated fusion. This did not improve, due to the presence of stiff wires and stent graft.
Conclusion: Automated image fusion was feasible when all vertebral edges were visible. Accuracy was non-inferior to manual image fusion regarding bone alignment. Future developments should focus on intraoperative image-based correction of vascular alignment.
Keywords: 2D-3D; 3D roadmap; Automated; EVAR; Fusion imaging; Image fusion; Navigation; Overlay.
© 2023. The Author(s).
Figures


References
-
- Nollert G, Hartkens T, Schwabenland I, Sunderbrink D, Dyck A. Hybrid operation theaters in vascular care: current and future technologies. In: Lanzer P, editor. PanVascular medicine. Berlin: Springer; 2015. pp. 4873–4889.
-
- Schwein A, Chinnadurai P, Behler G, Lumsden AB, Bismuth J, Bechara CF. Computed tomography angiography-fluoroscopy image fusion allows visceral vessel cannulation without angiography during fenestrated endovascular aneurysm repair. J Vasc Surg. 2018;68(1):2–11. doi: 10.1016/j.jvs.2017.11.062. - DOI - PubMed
-
- Doelare SAN, Smorenburg SPM, van Schaik TG, Blankensteijn JD, Wisselink W, Nederhoed JH, et al. Image fusion during standard and complex endovascular aortic repair, to fuse or not to fuse? A meta-analysis and additional data from a single-center retrospective cohort. J Endovas Ther. 2020;28:78–92. doi: 10.1177/1526602820960444. - DOI - PMC - PubMed
-
- Ahmad W, Hasselmann H-C, Galas N, Majd P, Brunkwall S, Brunkwall JS. Image fusion using the two-dimensional-three-dimensional registration method helps reduce contrast medium volume, fluoroscopy time, and procedure time in hybrid thoracic endovascular aortic repairs. J Vasc Surg. 2019;69(4):1003–1010. doi: 10.1016/j.jvs.2018.07.043. - DOI - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
