

Use of sodium-glucose cotransporter 2 inhibitors in Alberta adults with chronic kidney disease: a cross-sectional study identifying care gaps to inform knowledge translation
- PMID: 36720493
- PMCID: PMC9894653
- DOI: 10.9778/cmajo.20210281
Use of sodium-glucose cotransporter 2 inhibitors in Alberta adults with chronic kidney disease: a cross-sectional study identifying care gaps to inform knowledge translation
Abstract
Background: Sodium-glucose cotransporter 2 (SGLT2) inhibitors have important kidney and cardiovascular benefits in adults with chronic kidney disease. Among adults with diabetes, we characterized the prevalence of chronic kidney disease eligible for SGLT2 inhibitor treatment, based on definitions of eligibility from trials and diabetes guidelines, and assessed the predictors of SGLT2 inhibitor use.
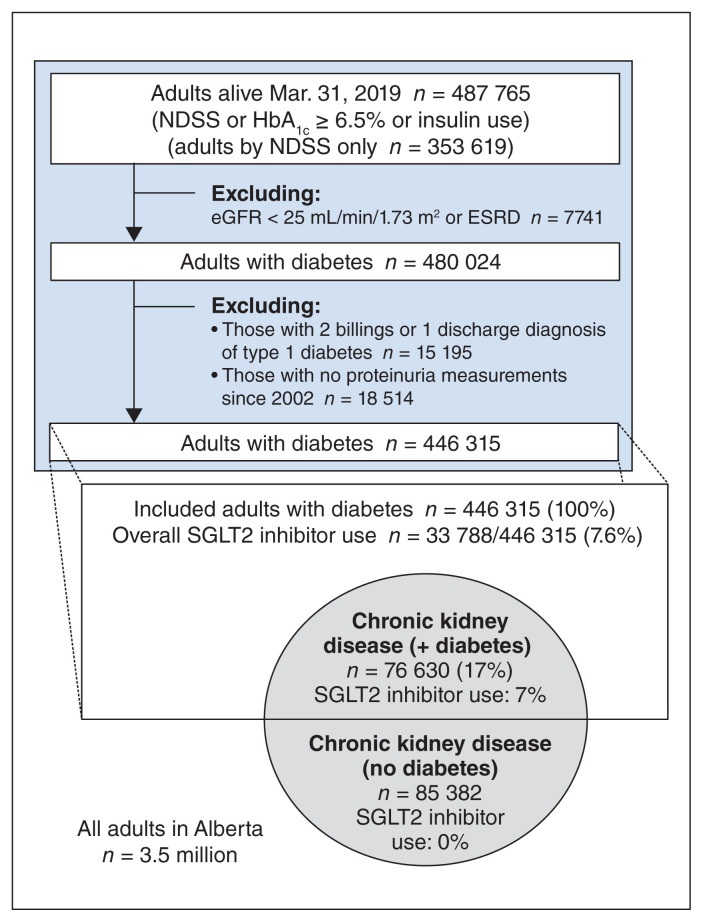
Methods: We conducted a cross-sectional study using linked administrative data from Alberta Health in adults with diabetes (2002-2019). Chronic kidney disease was defined as an estimated glomerular filtration rate (eGFR) less than 90 mL/min/1.73 m2 with severe or greater proteinuria (trial-based definition); or eGFR less than 60 mL/min/1.73 m2 or moderate or greater proteinuria regardless of eGFR (diabetes guideline-based definition). Predictors (sociodemographic characteristics, comorbidities and health care utilization) of SGLT2 inhibitor use were identified using logistic regression.
Results: Of 446 315 adults with diabetes, 76 630 (17.2%, guideline-based definition; 12 867 [2.9%], trial-based definition) had chronic kidney disease eligible for SGLT2 inhibitor treatment. A total of 7.1% used SGLT2 inhibitors. Older age, lower hemoglobin A1c (HbA1c) levels, female sex, lower neighbourhood income, rural residence and hospital admission were among variables associated with nonuse of SGLT2 inhibitors (adjusted odds ratios [ORs] from 0.13 [age ≥ 85 yr] to 0.92 [rural residence], p < 0.05). Family physician visits were associated with higher SGLT2 inhibitor use (adjusted OR 4.01, p < 0.001 for > 4 visits/yr). Considering all adults, both with and without diabetes, 162 012 individuals with chronic kidney disease (5% of all Alberta adults) may benefit from treatment with SGLT2 inhibitors.
Interpretation: Many adults with chronic kidney disease would derive heart and kidney benefits from treatment with SGLT2 inhibitors but had low SGLT2 inhibitor use as of 2019. Efforts will be needed to address lower use of SGLT2 inhibitors among female, older and lower-income adults, and to enhance primary care and promote awareness of the benefits of SGLT2 inhibitors independent of glycemic control.
© 2023 CMA Impact Inc. or its licensors.
Conflict of interest statement
Competing interests: Roseanne Yeung has previously received funding from the Novo Nordisk Alberta Diabetes Fund, a research grant administered by the University Hospital Foundation and Alberta Economic Development and Trade. Nairne Scott-Douglas has previously received research funding from Amgen and Bristol Myers Squibb. He has also received speaking honoraria and consulting fees from Amgen, Alexion, AstraZeneca, Janssen Pharmaceuticals, Novartis and Otsuka Pharmaceutical. Scott Klarenbach is co–scientific director of the Kidney Health Section of the Medicine Strategic Clinical Network, Alberta Health Services. No other competing interests were declared.
Figures
References
-
- Perkovic V, Jardine MJ, Neal B, et al. CREDENCE Trial Investigators. Canagliflozin and renal outcomes in type 2 diabetes and nephropathy. N Engl J Med. 2019;380:2295–306. - PubMed
-
- Heerspink HJL, Stefánsson BV, Correa-Rotter R, et al. DAPA-CKD Trial Committees and Investigators. Dapagliflozin in patients with chronic kidney disease. N Engl J Med. 2020;383:1436–46. - PubMed
-
- Navaneethan SD, Zoungas S, Caramori ML, et al. Diabetes management in chronic kidney disease: synopsis of the 2020 KDIGO clinical practice guideline. Ann Intern Med. 2021;174:385–94. - PubMed
-
- Diabetes Canada Clinical Practice Guidelines Expert Committee. Lipscombe L, Butalia S, Dasgupta K, et al. Pharmacologic glycemic management of type 2 diabetes in adults: 2020 update. Can J Diabetes. 2020;44:575–91. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous