

Effect of the GLP-1 receptor agonist semaglutide on metabolic disturbances in clozapine-treated or olanzapine-treated patients with a schizophrenia spectrum disorder: study protocol of a placebo-controlled, randomised clinical trial (SemaPsychiatry)
- PMID: 36720576
- PMCID: PMC9890830
- DOI: 10.1136/bmjopen-2022-068652
Effect of the GLP-1 receptor agonist semaglutide on metabolic disturbances in clozapine-treated or olanzapine-treated patients with a schizophrenia spectrum disorder: study protocol of a placebo-controlled, randomised clinical trial (SemaPsychiatry)
Abstract
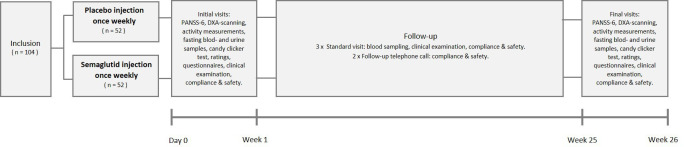
Introduction: Clozapine and olanzapine are some of the most effective antipsychotics, but both are associated with weight gain and relevant metabolic disturbances, including pre-diabetes and diabetes. Non-pharmacological/behavioural interventions have had limited effects counteracting these adverse effects. Semaglutide, a glucagon-like peptide 1 receptor agonist, is approved for the treatment of type 2 diabetes and obesity. We will investigate the long-term effects of add-on treatment with semaglutide once a week versus placebo once a week on the metabolic status in pre-diabetic (glycated haemoglobin A1c (HbA1c) 35-47 mmol/mol (5.4%-6.4%) and diabetic (HbA1c 48-57 mmol/mol (6.5%-7.4%)) patients diagnosed with a schizophrenia spectrum disorder who initiated clozapine or olanzapine treatment within the last 60 months.
Methods and analysis: This is a 26-week, double-blinded, randomised, placebo-controlled trial. Altogether, 104 patients diagnosed with a schizophrenia spectrum disorder, aged 18-65 years, with pre-diabetes or diabetes will be randomised to injections of 1.0 mg semaglutide once a week or placebo for 26 weeks. The primary endpoint is change from baseline in HbA1c. Secondary endpoints include changes in body weight, hip and waist circumference and plasma levels of insulin, glucagon, glucose, and C-peptide, insulin sensitivity, beta cell function, hepatic function, fibrosis-4 score, lipid profile, incretin hormones, bone markers, body composition, bone density, proteomic analyses and oxidative stress markers. Together with alcohol, tobacco and drug use, potential effects on the reward value of a sweet-fat stimulus, psychopathology, level of activity and quality of life will also be assessed.
Ethics and dissemination: This study is approved by the Danish Medicines Agency and the regional scientific ethics committee of the Capital Region of Denmark (committee C, #H-20019008) and will be carried out in accordance with International Council for Harmonisation Good Clinical Practice guidelines and the Helsinki Declaration. The results will be disseminated through peer-review publications and conference presentations.
Trial registration number: NCT04892199.
Keywords: Adult psychiatry; DIABETES & ENDOCRINOLOGY; MENTAL HEALTH; PSYCHIATRY; Schizophrenia & psychotic disorders.
© Author(s) (or their employer(s)) 2023. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: AFJ received an unrestricted research grant from Novo Nordisk A/S for the present clinical study. TV served on scientific advisory panels and/or speaker's bureaus for Amgen, AstraZeneca, Boehringer Ingelheim, Bristol-Myers Squibb, Eli Lilly, Gilead, GSK, Merck Sharp & Dohme, Mundipharma, Novo Nordisk, Sanofi and Sun Pharma. TV served as a consultant to and/or received research support from Amgen, AstraZeneca, Boehringer Ingelheim, Bristol-Myers Squibb, Eli Lilly, Gilead, GSK, Merck Sharp & Dohme, Mundipharma, Novo Nordisk, Sanofi and Sun Pharma. HS served on scientific advisory panels for Boehringer Ingelheim and Novo Nordisk. CUC has been a consultant and/or advisor to or has received honoraria from AbbVie, Acadia, Alkermes, Allergan, Angelini, Aristo, Boehringer-Ingelheim, Cardio Diagnostics, Cerevel, CNX Therapeutics, Compass Pathways, Darnitsa, Gedeon Richter, Hikma, Holmusk, IntraCellular Therapies, Janssen/J&J, Karuna, LB Pharma, Lundbeck, MedAvante-ProPhase, MedInCell, Merck, Mindpax, Mitsubishi Tanabe Pharma, Mylan, Neurocrine, Newron, Noven, Otsuka, Pharmabrain, PPD Biotech, Recordati, Relmada, Reviva, Rovi, Seqirus, SK Life Science, Sunovion, Sun Pharma, Supernus, Takeda, Teva and Viatris. He provided expert testimony for Janssen and Otsuka. He served on a Data Safety Monitoring Board for Lundbeck, Relmada, Reviva, Rovi, Supernus, and Teva. He has received grant support from Janssen and Takeda. He received royalties from UpToDate and is also a stock option holder of Cardio Diagnostics, Mindpax, LB Pharma and Quantic. OKF reports speaker fees for Lundbeck Pharma A/S and consultant work for WCG Clinical. FKK served on scientific advisory panels and/or been part of speaker’s bureaus for, served as a consultant to and/or received research support from Amgen, AstraZeneca, Boehringer Ingelheim, Eli Lilly, MSD/Merck, Mundipharma, Norgine, Novo Nordisk, Sanofi and Zealand Pharma. MV received consultancy fees from Lundbeck and Janssen-Cilag. AAD received a speaker honorarium from Otsuka Pharmaceutical. MRS has nothing to disclose. Novo Nordisk A/S commented on the study design but will not influence trial conduction, data analysis, interpretation or publication. All data are owned by the authors, who all have full data access.
Figures
Similar articles
-
Does a GLP-1 receptor agonist change glucose tolerance in patients treated with antipsychotic medications? Design of a randomised, double-blinded, placebo-controlled clinical trial.BMJ Open. 2014 Mar 25;4(3):e004227. doi: 10.1136/bmjopen-2013-004227. BMJ Open. 2014. PMID: 24667381 Free PMC article. Clinical Trial.
-
Home-based Intervention with Semaglutide Treatment of Neuroleptic-Related Prediabetes (HISTORI): protocol describing a prospective, randomised, placebo controlled and double-blinded multicentre trial.BMJ Open. 2024 Mar 18;14(3):e077173. doi: 10.1136/bmjopen-2023-077173. BMJ Open. 2024. PMID: 38503415 Free PMC article.
-
Effect of Liraglutide Treatment on Prediabetes and Overweight or Obesity in Clozapine- or Olanzapine-Treated Patients With Schizophrenia Spectrum Disorder: A Randomized Clinical Trial.JAMA Psychiatry. 2017 Jul 1;74(7):719-728. doi: 10.1001/jamapsychiatry.2017.1220. JAMA Psychiatry. 2017. PMID: 28601891 Free PMC article. Clinical Trial.
-
[Antipsychotics in bipolar disorders].Encephale. 2004 Sep-Oct;30(5):417-24. doi: 10.1016/s0013-7006(04)95456-5. Encephale. 2004. PMID: 15627046 Review. French.
-
Comparing once-weekly semaglutide to incretin-based therapies in patients with type 2 diabetes: a systematic review and meta-analysis.Diabetes Metab. 2019 Apr;45(2):102-109. doi: 10.1016/j.diabet.2018.09.002. Epub 2018 Sep 20. Diabetes Metab. 2019. PMID: 30243806
Cited by
-
Metabolic syndrome in patients with schizophrenia: Underlying mechanisms and therapeutic approaches (Review).Mol Med Rep. 2025 May;31(5):114. doi: 10.3892/mmr.2025.13479. Epub 2025 Feb 28. Mol Med Rep. 2025. PMID: 40017113 Free PMC article. Review.
-
The Combined Effects of EEG Biofeedback and Olanzapine on Glucose and Lipid Metabolism, Cardiac Function, and Cognitive Function in Patients With Schizophrenia.Actas Esp Psiquiatr. 2025 May;53(3):570-577. doi: 10.62641/aep.v53i3.1823. Actas Esp Psiquiatr. 2025. PMID: 40356004 Free PMC article.
-
Interaction of Semaglutide and Ziprasidone in a Patient With Schizophrenia: A Case Report.Cureus. 2024 Apr 29;16(4):e59319. doi: 10.7759/cureus.59319. eCollection 2024 Apr. Cureus. 2024. PMID: 38817502 Free PMC article.
-
A comprehensive review on schizophrenia: epidemiology, pathogenesis, diagnosis, conventional treatments, and proposed natural compounds used for management.Naunyn Schmiedebergs Arch Pharmacol. 2025 Jun 13. doi: 10.1007/s00210-025-04351-0. Online ahead of print. Naunyn Schmiedebergs Arch Pharmacol. 2025. PMID: 40512218 Review.
-
Antidepressants and Weight Gain: An Update on the Evidence and Clinical Implications.Curr Obes Rep. 2025 Jan 3;14(1):2. doi: 10.1007/s13679-024-00598-5. Curr Obes Rep. 2025. PMID: 39753939 Review.
References
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical