

Microbial transmission, colonisation and succession: from pregnancy to infancy
- PMID: 36720630
- PMCID: PMC10086306
- DOI: 10.1136/gutjnl-2022-328970
Microbial transmission, colonisation and succession: from pregnancy to infancy
Abstract
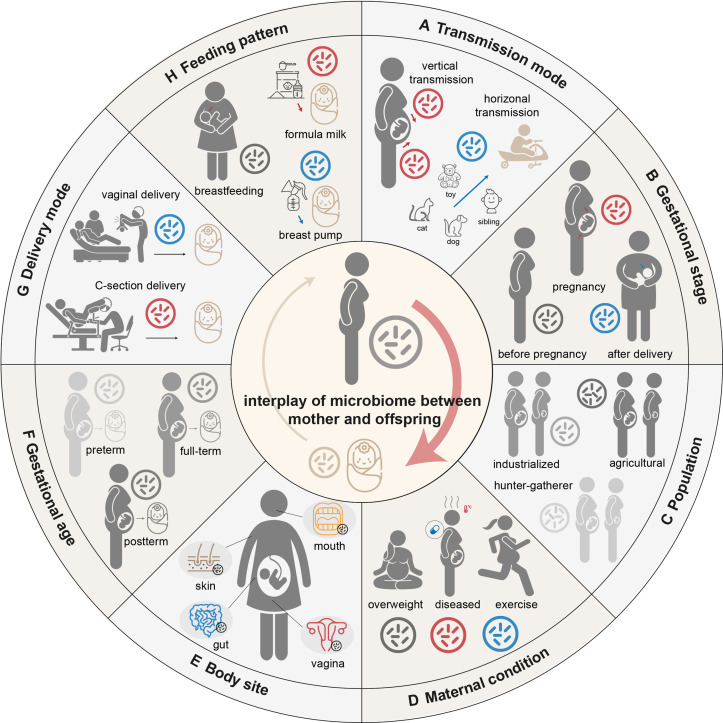
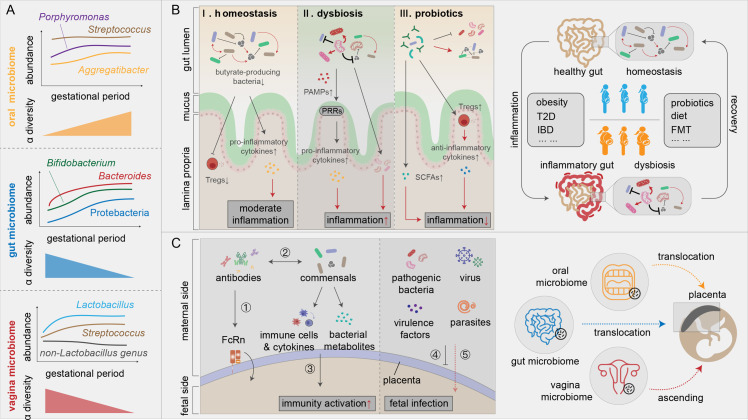
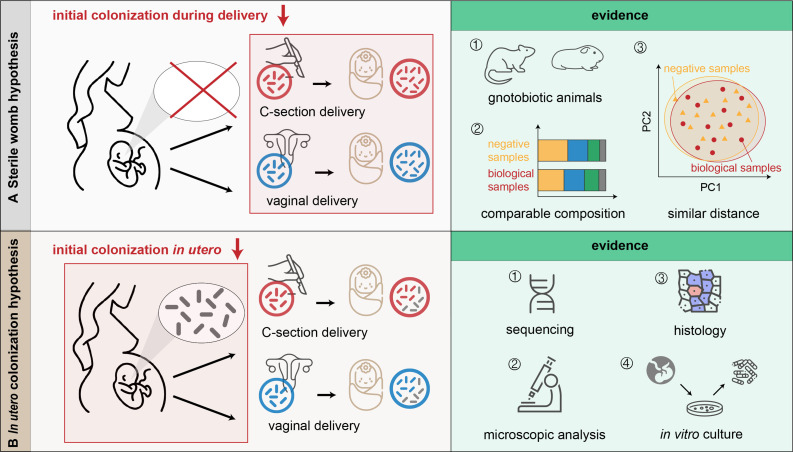
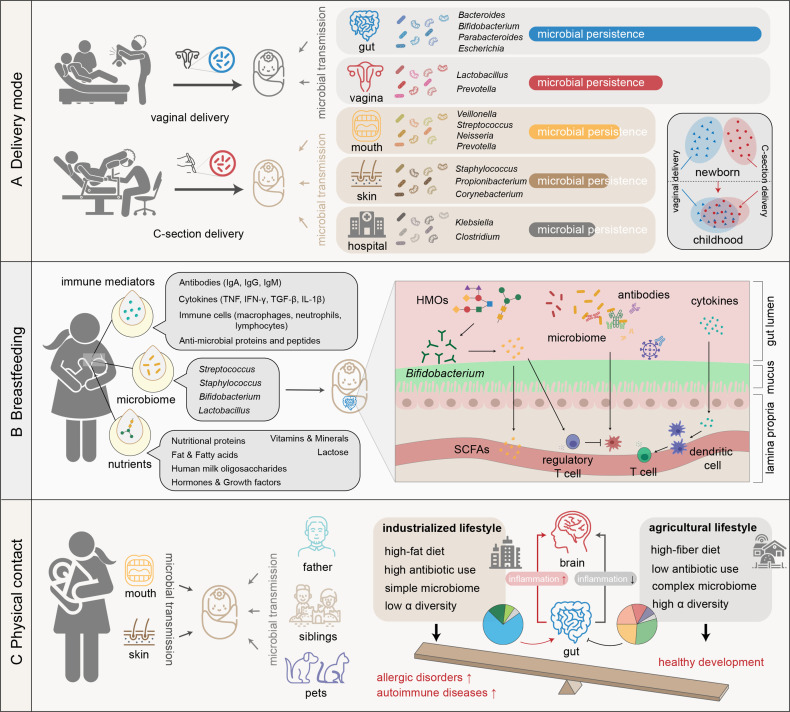
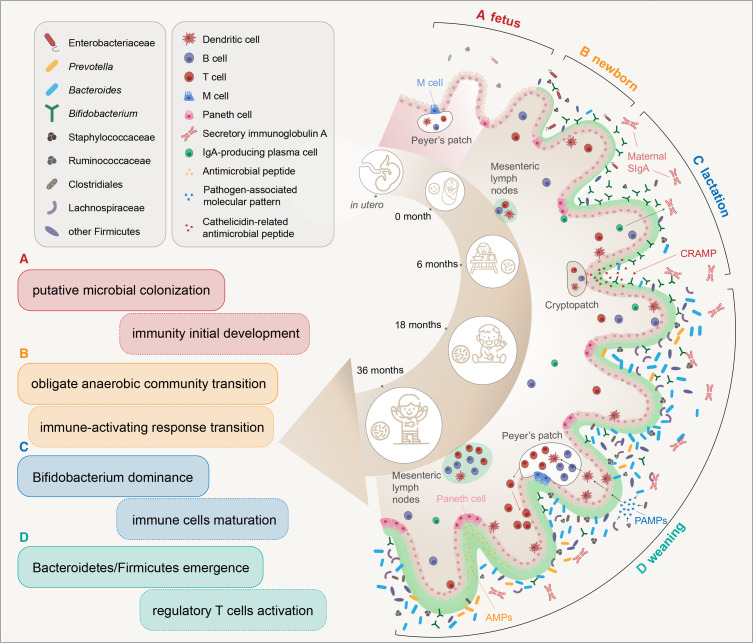
The microbiome has been proven to be associated with many diseases and has been used as a biomarker and target in disease prevention and intervention. Currently, the vital role of the microbiome in pregnant women and newborns is increasingly emphasised. In this review, we discuss the interplay of the microbiome and the corresponding immune mechanism between mothers and their offspring during the perinatal period. We aim to present a comprehensive picture of microbial transmission and potential immune imprinting before and after delivery. In addition, we discuss the possibility of in utero microbial colonisation during pregnancy, which has been highly debated in recent studies, and highlight the importance of the microbiome in infant development during the first 3 years of life. This holistic view of the role of the microbial interplay between mothers and infants will refine our current understanding of pregnancy complications as well as diseases in early life and will greatly facilitate the microbiome-based prenatal diagnosis and treatment of mother-infant-related diseases.
Keywords: infant gut; intestinal development; intestinal microbiology.
© Author(s) (or their employer(s)) 2023. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical