

Minimizing population health loss due to scarcity in OR capacity: validation of quality of life input
- PMID: 36721106
- PMCID: PMC9887555
- DOI: 10.1186/s12874-022-01818-z
Minimizing population health loss due to scarcity in OR capacity: validation of quality of life input
Abstract
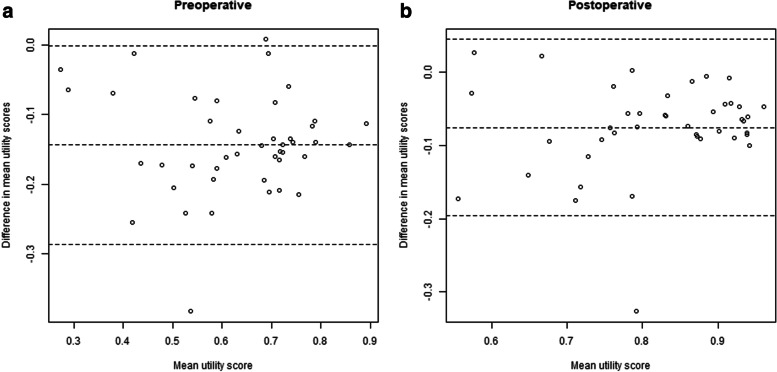
Objectives: A previously developed decision model to prioritize surgical procedures in times of scarce surgical capacity used quality of life (QoL) primarily derived from experts in one center. These estimates are key input of the model, and might be more context-dependent than the other input parameters (age, survival). The aim of this study was to validate our model by replicating these QoL estimates.
Methods: The original study estimated QoL of patients in need of commonly performed procedures in live expert-panel meetings. This study replicated this procedure using a web-based Delphi approach in a different hospital. The new QoL scores were compared with the original scores using mixed effects linear regression. The ranking of surgical procedures based on combined QoL values from the validation and original study was compared to the ranking based solely on the original QoL values.
Results: The overall mean difference in QoL estimates between the validation study and the original study was - 0.11 (95% CI: -0.12 - -0.10). The model output (DALY/month delay) based on QoL data from both studies was similar to the model output based on the original data only: The Spearman's correlation coefficient between the ranking of all procedures before and after including the new QoL estimates was 0.988.
Discussion: Even though the new QoL estimates were systematically lower than the values from the original study, the ranking for urgency based on health loss per unit of time delay of procedures was consistent. This underscores the robustness and generalizability of the decision model for prioritization of surgical procedures.
Keywords: Decision modeling; Prioritization; Quality of life; Surgery; Validation; Value based health care.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures




References
-
- Tan W, Aboulhosn J. The cardiovascular burden of coronavirus disease 2019 (COVID-19) with a focus on congenital heart disease. Int J Cardiol. 2020 Jun;309:70–7 Available from: https://pubmed.ncbi.nlm.nih.gov/32248966/. - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
