

Effect of a computerized decision support system on the treatment approach of stage III or IV pressure injury in patients with spinal cord injury: a feasibility study
- PMID: 36721265
- PMCID: PMC9890825
- DOI: 10.1186/s12913-023-09045-y
Effect of a computerized decision support system on the treatment approach of stage III or IV pressure injury in patients with spinal cord injury: a feasibility study
Abstract
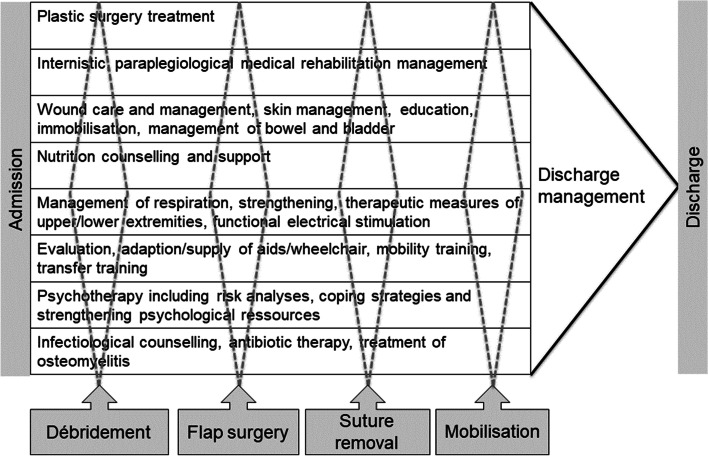
Background: Stage III and IV pressure injuries (PIs) in patients with spinal cord injury (SCI) require complex interdisciplinary and interprofessional treatment approaches that are difficult to implement. Practical aspects, such as information exchange and coordination, remain challenging. We investigated whether a computerized decision support system (CDSS) could increase treatment adherence and improve clinical outcomes and interprofessional collaboration.
Method: In this feasibility study, a core team developed the initial treatment process and adapted it based on several discussions with clinical experts and information technologists. The CDSS followed the Basel Decubitus Approach and was used in a clinic specializing in SCI. Thirty patients with SCI admitted for stage III/IV PI between July 2016 and May 2017 were randomly allocated to standard or CDSS-supported care. Between-group differences in treatment adherence, complication rates, length of stay, and costs were analyzed using descriptive statistics. The use of the CDSS and potential barriers and facilitators were evaluated through interprofessional focus groups, transcribed verbatim, and thematically analyzed (30 participants).
Results: No differences in SCI characteristics, comorbidities, or PI characteristics (localization: ischium [number (n) = 19 PI, 63%], sacrum [n = 10 PI, 33%], recurrent PI [n = 21, 70%]) were found between the two groups. Furthermore, no statistically significant differences were observed in treatment adherence, frequency of major (20% vs. 13% between CDSS and control group) and minor (33% vs 27%) complications, and length of stay (98 [±28] vs 81 [±23] days). Healthcare professionals found the CDSS to be helpful for visualizing the treatment process. However, the high workload and difficulties in the information technology processes, such as missing reminders, slow computer performance and data processing, and poor accessibility, hindered the effective implementation of the CDSS.
Conclusion: The implementation of the CDSS to support the treatment of stage III/IV PI in patients with SCI was feasible and included definitions of milestones, interventions, and outcomes. However, to assess the impact of the CDSS, a longer observation period is required. Further, the technical difficulties must be addressed, and solid integration of the CDSS into the clinical information system is necessary.
Trial registration: This quality improvement project received a declaration of no objection from the Ethics Committee of Northwest and Central Switzerland (EKNZ UBE-16/003), and ethical approval was received for the focus groups (EKNZ Req-2017-00860).
Keywords: Basel Decubitus Approach; Clinical Decision Support Systems; Computer Systems; Interprofessional Collaboration; Pressure Injury; Process Management; Rehabilitation; Spinal Cord Injury.
© 2023. The Author(s).
Conflict of interest statement
All authors declared no conflicts of interest.
Figures
Similar articles
-
Treatment and cost of pressure injury stage III or IV in four patients with spinal cord injury: the Basel Decubitus Concept.Spinal Cord Ser Cases. 2019 Mar 15;5:30. doi: 10.1038/s41394-019-0173-0. eCollection 2019. Spinal Cord Ser Cases. 2019. PMID: 31632697 Free PMC article.
-
Risk factors of major complications after flap surgery in the treatment of stage III and IV pressure injury in people with spinal cord injury/disorder: a retrospective cohort study.Spinal Cord. 2024 Jan;62(1):34-41. doi: 10.1038/s41393-023-00944-9. Epub 2023 Dec 20. Spinal Cord. 2024. PMID: 38123748 Free PMC article.
-
Implementation of Pressure Injury Prevention Best Practices Across 6 Canadian Rehabilitation Sites: Results From the Spinal Cord Injury Knowledge Mobilization Network.Arch Phys Med Rehabil. 2019 Feb;100(2):327-335. doi: 10.1016/j.apmr.2018.07.444. Epub 2018 Nov 9. Arch Phys Med Rehabil. 2019. PMID: 30419231
-
Treatment approaches of stage III and IV pressure injury in people with spinal cord injury: A scoping review.J Spinal Cord Med. 2023 Sep;46(5):705-715. doi: 10.1080/10790268.2022.2108645. Epub 2022 Sep 21. J Spinal Cord Med. 2023. PMID: 36129337 Free PMC article.
-
Clinical practice, decision-making, and use of clinical decision support systems in invasive mechanical ventilation: a narrative review.Br J Anaesth. 2024 Jul;133(1):164-177. doi: 10.1016/j.bja.2024.03.011. Epub 2024 Apr 17. Br J Anaesth. 2024. PMID: 38637268 Free PMC article. Review.
References
-
- Rotter T, Kinsman L, James E, Machotta A, Gothe H, Willis J, et al. Clinical pathways: effects on professional practice, patient outcomes, length of stay and hospital costs. Cochrane Database Syst Rev. 2010;(3):CD006632. 10.1002/14651858.CD006632.pub2. PMID: 20238347. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
