

Fixation of Hand Fractures with Intramedullary Headless Compression Screws
- PMID: 36721649
- PMCID: PMC9846723
- DOI: 10.22038/ABJS.2022.64506.3102
Fixation of Hand Fractures with Intramedullary Headless Compression Screws
Abstract
Metacarpal and phalangeal fractures remain among the most frequently encountered orthopedic injuries, accounting for 10% of all fractures. For operative fractures, there is an array of treatment options with percutaneous kirschner wire stabilization and screw and plate fixation strategies predominating. Recently, a new fixation method was introduced, intramedullary (IM) fixation with headless screws, which has advantages of a percutaneous technique and buried hardware. The purpose of this review is to highlight the indications and surgical techniques of IM screw fixation of metacarpal and phalangeal fractures. Although more research is needed, IM fixation represents a potentially reliable alternative to Kirschner-wire and plate fixation.
Keywords: Indications; Intramedullary compression; Metacarpal fracture; Phalanx fracture; Technique.
2022 © BY THE ARCHIVES OF BONE AND JOINT SURGERY.
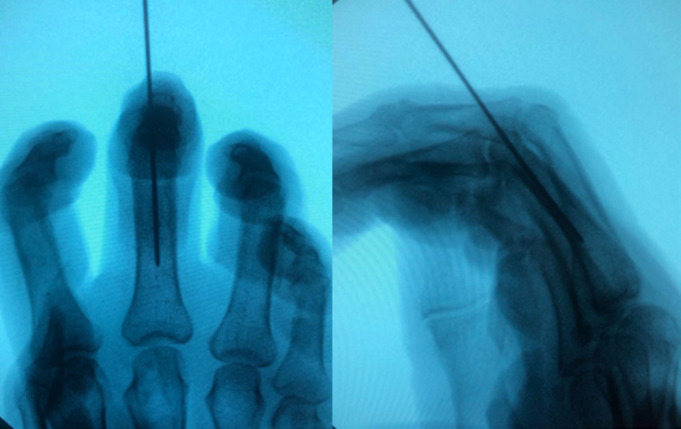
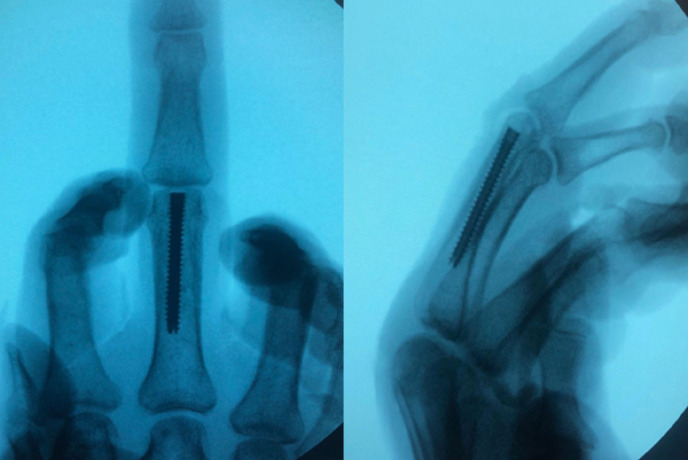
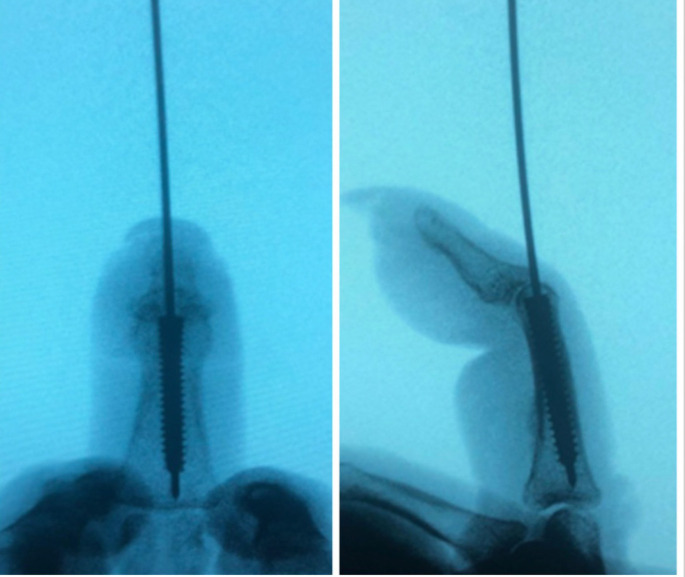
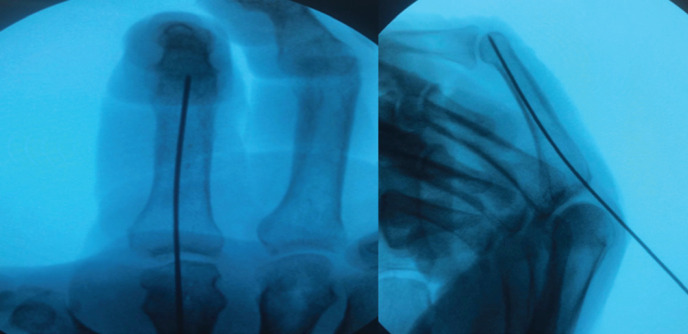
Figures








References
-
- Gajendran VK, Gajendran VK, Malone KJ. Management of complications with hand fractures. Hand Clin. 2015;31(2):165–177. - PubMed
-
- Cotterell IH, Richard MJ. Metacarpal and phalangeal fractures in athletes. Clin Sports Med. 2015;34(1):69–98. - PubMed
-
- Henry MH. Fractures of the proximal phalanx and metacarpals in the hand: preferred methods of stabilization. J Am Acad Orthop Surg. 2008;16(10):586–595. - PubMed
-
- Zyluk A, Budzyński T. Treatment of metacarpal and phalangeal fractures--a review. Chir Narzadow Ruchu Ortop Pol. 2006;71(4):299–308. - PubMed
-
- Kozin SH, Thoder JJ, Lieberman G. Operative treatment of metacarpal and phalangeal shaft fractures. J Am Acad Orthop Surg. 2000;8(2):111–121. - PubMed
Publication types
LinkOut - more resources
Full Text Sources