

Risk of Reoperation for Recurrence After Elective Primary Groin and Ventral Hernia Repair by Supervised Residents
- PMID: 36723916
- PMCID: PMC10099066
- DOI: 10.1001/jamasurg.2022.7502
Risk of Reoperation for Recurrence After Elective Primary Groin and Ventral Hernia Repair by Supervised Residents
Abstract
Importance: Surgical training involves letting residents operate under supervision. Since hernia repair is a common procedure worldwide, it is a frequent part of the surgical curriculum.
Objective: To assess the risk of reoperation for recurrence after elective primary groin and ventral hernia repair performed by supervised residents compared with that by specialists.
Design, setting, and participants: This nationwide register-based cohort study included data from January 2016 to September 2021. Patients were followed up until reoperation, emigration, death, or the end of the study period. The study used data from the Danish Inguinal and Ventral Hernia Databases linked with data from the Danish Patient Safety Authority's Online Register via surgeons' unique authorization ID. The cohort included patients aged 18 years or older who underwent primary elective hernia repairs performed by supervised residents or specialists for inguinal, femoral, epigastric, or umbilical hernias. Hernia repairs were divided into the following 4 groups: Lichtenstein groin, laparoscopic transabdominal preperitoneal (TAPP) groin, open ventral, and laparoscopic ventral.
Exposures: Hernia repairs performed by supervised residents vs specialists.
Main outcomes and measures: Reoperation for recurrence, analyzed separately for all 4 groups.
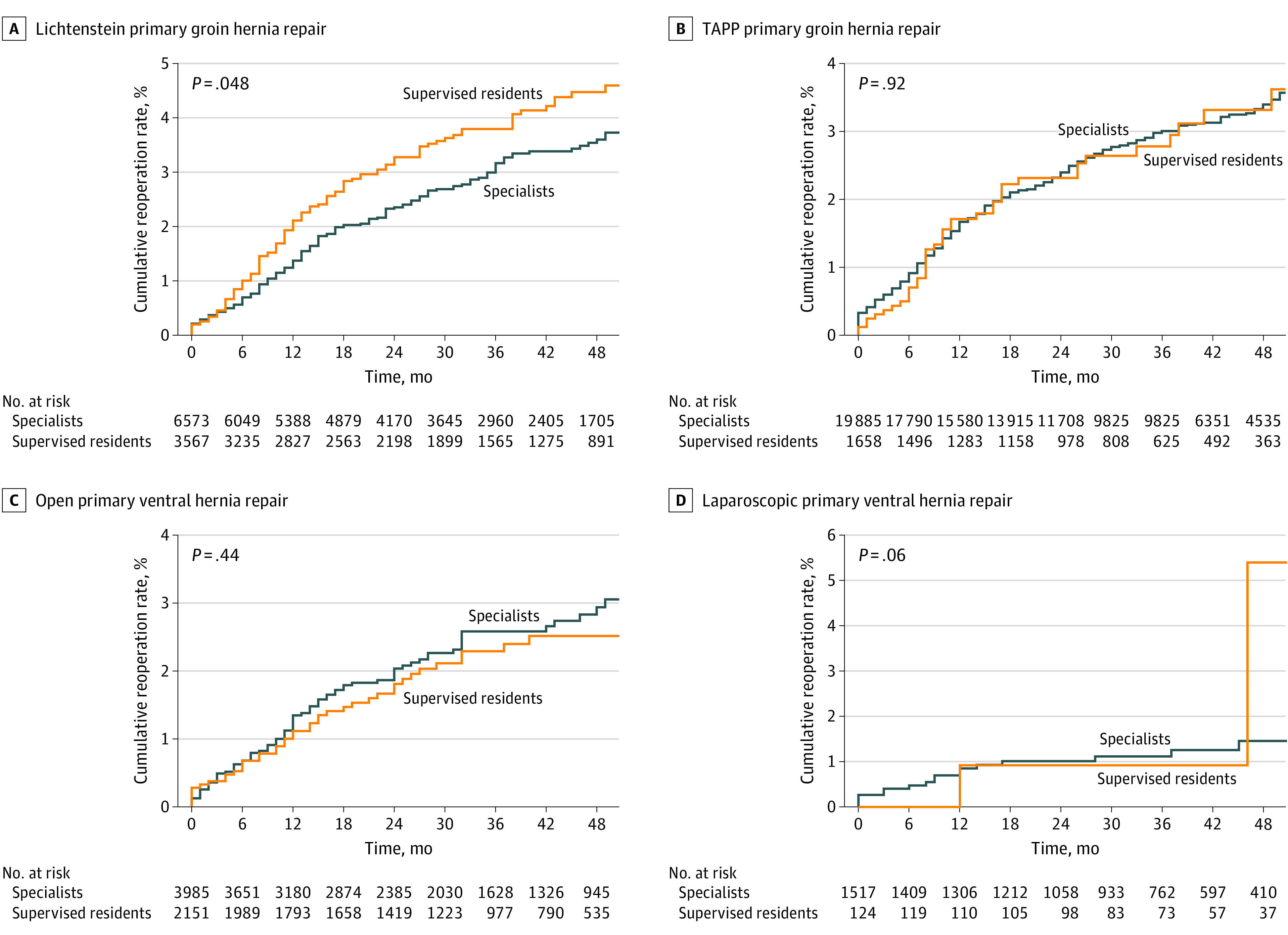
Results: A total of 868 specialists and residents who performed 31 683 primary groin and 7777 primary ventral hernia repairs were included in this study. The median age of patients who underwent hernia repair was 60 years (IQR, 48-70 years), and 33 424 patients (84.7%) were male. There was no significant difference in the adjusted risk of reoperation after Lichtenstein groin hernia repair (hazard ratio [HR], 1.26; 95% CI, 0.99-1.59), laparoscopic groin hernia repair (HR, 1.01; 95% CI, 0.73-1.40), open ventral hernia repair (HR, 0.89; 95% CI, 0.61-1.29), and laparoscopic ventral hernia repair (HR, 2.96; 95% CI, 0.99-8.84) performed by supervised residents compared with those by specialists. There was, however, a slightly increased unadjusted, cumulative reoperation rate after Lichtenstein repairs performed by supervised residents compared with those by specialists (4.8% vs 4.2%; P = .048).
Conclusions and relevance: The findings of this study suggest that neither open nor laparoscopic repair of groin and ventral hernias performed by supervised residents appeared to be associated with a higher risk of reoperation for recurrence compared with the operations performed by specialists. This indicates that residents may safely perform elective hernia repair when supervised as part of their training curriculum.
Conflict of interest statement
Figures

Comment in
-
Supervision and Transparency in Resident Training.JAMA Surg. 2023 Apr 1;158(4):367. doi: 10.1001/jamasurg.2022.7513. JAMA Surg. 2023. PMID: 36723954 No abstract available.
