

Reports of Guillain-Barré Syndrome After COVID-19 Vaccination in the United States
- PMID: 36723942
- PMCID: PMC9892957
- DOI: 10.1001/jamanetworkopen.2022.53845
Reports of Guillain-Barré Syndrome After COVID-19 Vaccination in the United States
Erratum in
-
Errors in Abstract, Results, and Discussion.JAMA Netw Open. 2023 May 1;6(5):e2315740. doi: 10.1001/jamanetworkopen.2023.15740. JAMA Netw Open. 2023. PMID: 37171824 Free PMC article. No abstract available.
Abstract
Importance: Because of historical associations between vaccines and Guillain-Barré syndrome (GBS), the condition was a prespecified adverse event of special interest for COVID-19 vaccine monitoring.
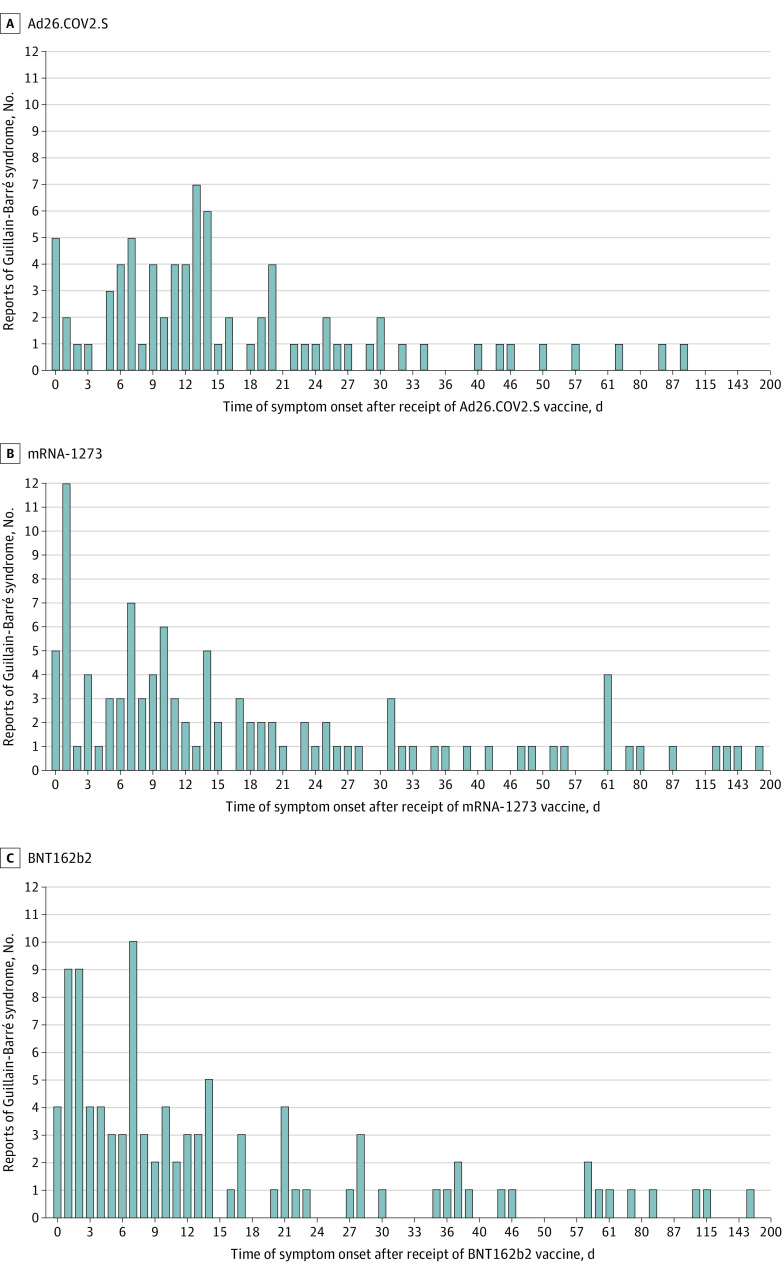
Objective: To evaluate GBS reports to the Vaccine Adverse Event Reporting System (VAERS) and compare reporting patterns within 21 and 42 days after vaccination with Ad26.COV2.S (Janssen), BNT162b2 (Pfizer-BioNTech), and mRNA-1273 (Moderna) COVID-19 vaccines.
Design, setting, and participants: This retrospective cohort study was conducted using US VAERS reports submitted during December 2020 to January 2022. GBS case reports verified as meeting the Brighton Collaboration case definition for GBS in US adults after COVID-19 vaccination were included.
Exposures: Receipt of the Ad26.COV2.S, BNT162b2, or mRNA-1273 COVID-19 vaccine.
Main outcomes and measures: Descriptive analyses of GBS case were conducted. GBS reporting rates within 21 and 42 days after Ad26.COV2.S, BNT162b2, or mRNA-1273 vaccination based on doses administered were calculated. Reporting rate ratios (RRRs) after receipt of Ad26.COV2.S vs BNT162b2 or mRNA-1273 within 21- and 42-day postvaccination intervals were calculated. Observed-to-expected (OE) ratios were estimated using published GBS background rates.
Results: Among 487 651 785 COVID-19 vaccine doses, 17 944 515 doses (3.7%) were Ad26.COV2.S, 266 859 784 doses (54.7%) were BNT162b2, and 202 847 486 doses (41.6%) were mRNA-1273. Of 295 verified reports of individuals with GBS identified after COVID-19 vaccination (12 Asian [4.1%], 18 Black [6.1%], and 193 White [65.4%]; 17 Hispanic [5.8%]; 169 males [57.3%]; median [IQR] age, 59.0 [46.0-68.0] years), 275 reports (93.2%) documented hospitalization. There were 209 and 253 reports of GBS that occurred within 21 days and 42 days of vaccination, respectively. Within 21 days of vaccination, GBS reporting rates per 1 000 000 doses were 3.29 for Ad26.COV.2, 0.29 for BNT162b2, and 0.35 for mRNA-1273 administered; within 42 days of vaccination, they were 4.07 for Ad26.COV.2, 0.34 for BNT162b2, and 0.44 for mRNA-1273. GBS was more frequently reported within 21 days after Ad26.COV2.S than after BNT162b2 (RRR = 11.40; 95% CI, 8.11-15.99) or mRNA-1273 (RRR = 9.26; 95% CI, 6.57-13.07) vaccination; similar findings were observed within 42 days after vaccination (BNT162b2: RRR = 12.06; 95% CI, 8.86-16.43; mRNA-1273: RRR = 9.27; 95% CI, 6.80-12.63). OE ratios were 3.79 (95% CI, 2.88-4.88) for 21-day and 2.34 (95% CI, 1.83-2.94) for 42-day intervals after Ad26.COV2.S vaccination and less than 1 (not significant) after BNT162b2 and mRNA-1273 vaccination within both postvaccination periods.
Conclusions and relevance: This study found disproportionate reporting and imbalances after Ad26.COV2.S vaccination, suggesting that Ad26.COV2.S vaccination was associated with increased risk for GBS. No associations between mRNA COVID-19 vaccines and risk of GBS were observed.
Conflict of interest statement
Figures
References
-
- Sejvar JJ, Kohl KS, Gidudu J, et al. ; Brighton Collaboration GBS Working Group . Guillain-Barré syndrome and Fisher syndrome: case definitions and guidelines for collection, analysis, and presentation of immunization safety data. Vaccine. 2011;29(3):599-612. doi: 10.1016/j.vaccine.2010.06.003 - DOI - PubMed
-
- Centers for Disease Control and Prevention . Guillain-Barré Syndrome and vaccines. Accessed May 21, 2022. https://www.cdc.gov/vaccinesafety/concerns/guillain-barre-syndrome.html
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
