

Prophylactic Administration of Mesenchymal Stromal Cells Does Not Prevent Arrested Lung Development in Extremely Premature-Born Non-Human Primates
- PMID: 36724000
- PMCID: PMC9985113
- DOI: 10.1093/stcltm/szac088
Prophylactic Administration of Mesenchymal Stromal Cells Does Not Prevent Arrested Lung Development in Extremely Premature-Born Non-Human Primates
Abstract
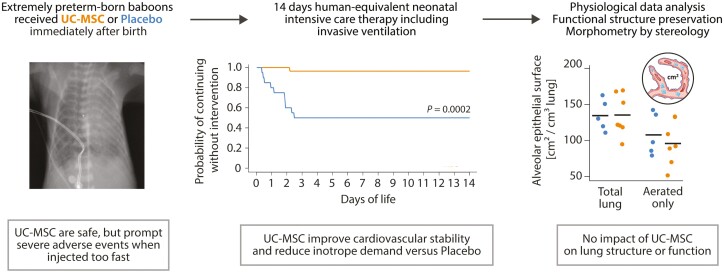
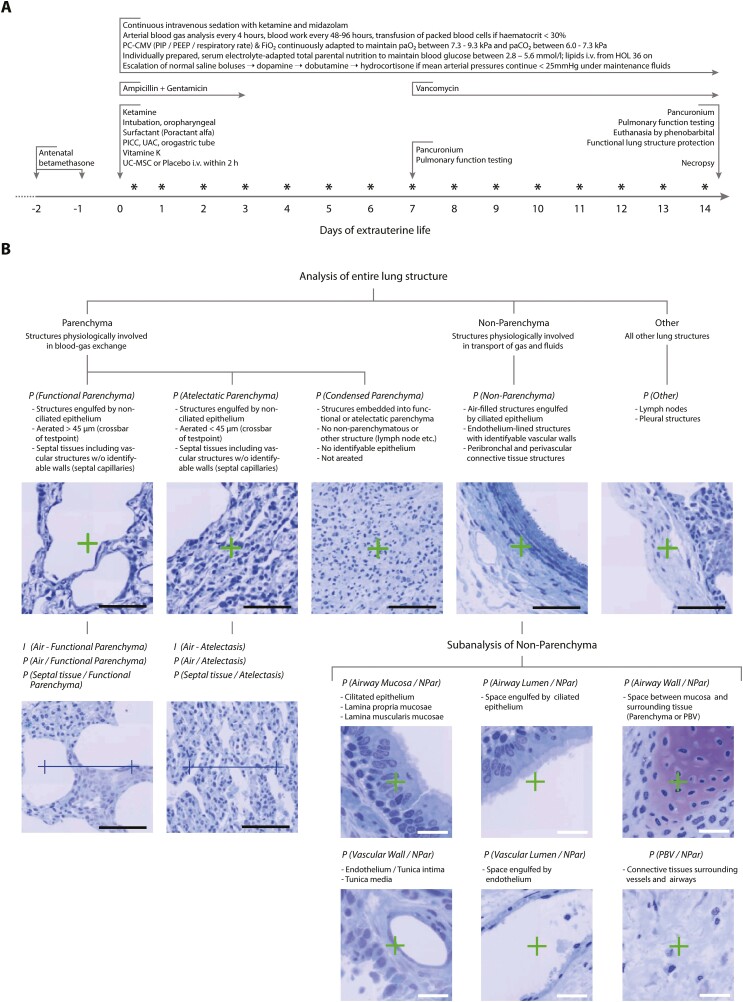
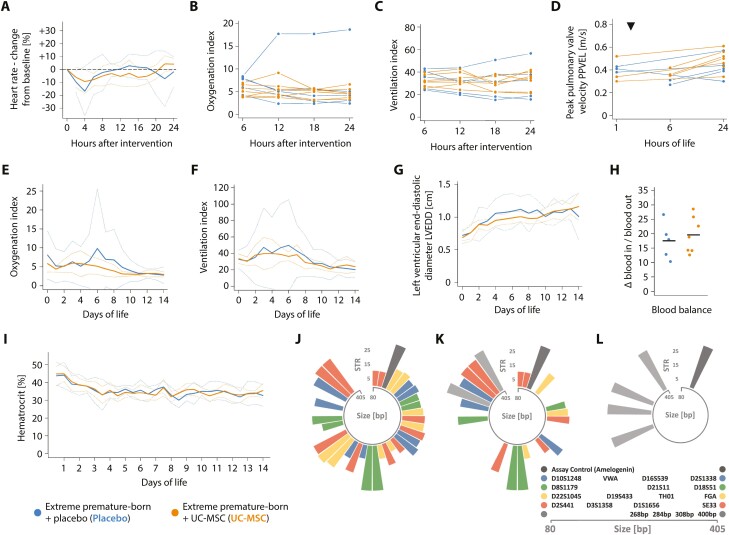
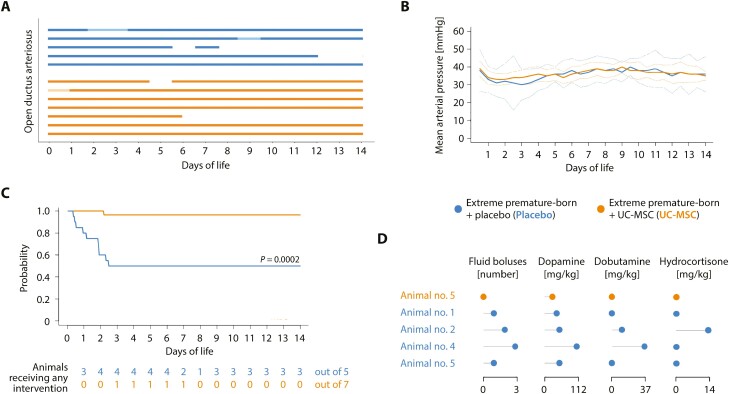
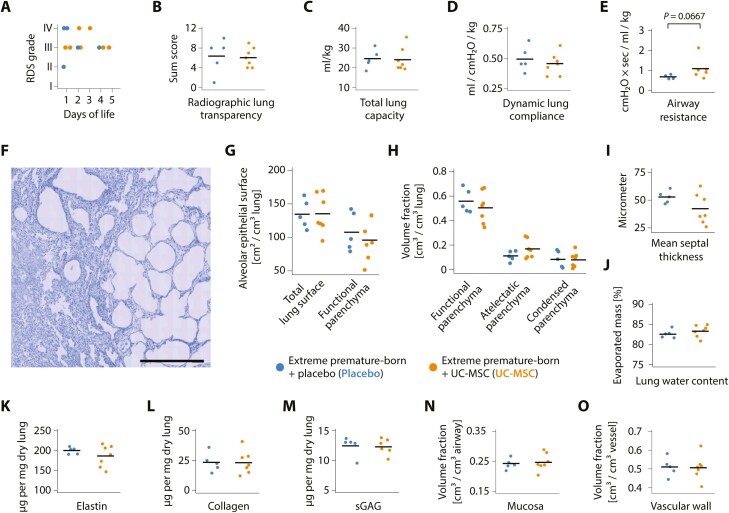
Premature birth is a leading cause of childhood morbidity and mortality and often followed by an arrest of postnatal lung development called bronchopulmonary dysplasia. Therapies using exogenous mesenchymal stromal cells (MSC) have proven highly efficacious in term-born rodent models of this disease, but effects of MSC in actual premature-born lungs are largely unknown. Here, we investigated thirteen non-human primates (baboons; Papio spp.) that were born at the limit of viability and given a single, intravenous dose of ten million human umbilical cord tissue-derived MSC per kilogram or placebo immediately after birth. Following two weeks of human-equivalent neonatal intensive care including mechanical ventilation, lung function testing and echocardiographic studies, lung tissues were analyzed using unbiased stereology. We noted that therapy with MSC was feasible, safe and without signs of engraftment when administered as controlled infusion over 15 minutes, but linked to adverse events when given faster. Administration of cells was associated with improved cardiovascular stability, but neither benefited lung structure, nor lung function after two weeks of extrauterine life. We concluded that a single, intravenous administration of MSC had no short- to mid-term lung-protective effects in extremely premature-born baboons, sharply contrasting data from term-born rodent models of arrested postnatal lung development and urging for investigations on the mechanisms of cell-based therapies for diseases of prematurity in actual premature organisms.
Keywords: adverse events; bronchopulmonary dysplasia; cell therapy; extreme premature birth; lung development; unbiased stereology.
© The Author(s) 2023. Published by Oxford University Press.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
