

NRF2 Activation Reprograms Defects in Oxidative Metabolism to Restore Macrophage Function in Chronic Obstructive Pulmonary Disease
- PMID: 36724365
- PMCID: PMC7614437
- DOI: 10.1164/rccm.202203-0482OC
NRF2 Activation Reprograms Defects in Oxidative Metabolism to Restore Macrophage Function in Chronic Obstructive Pulmonary Disease
Abstract
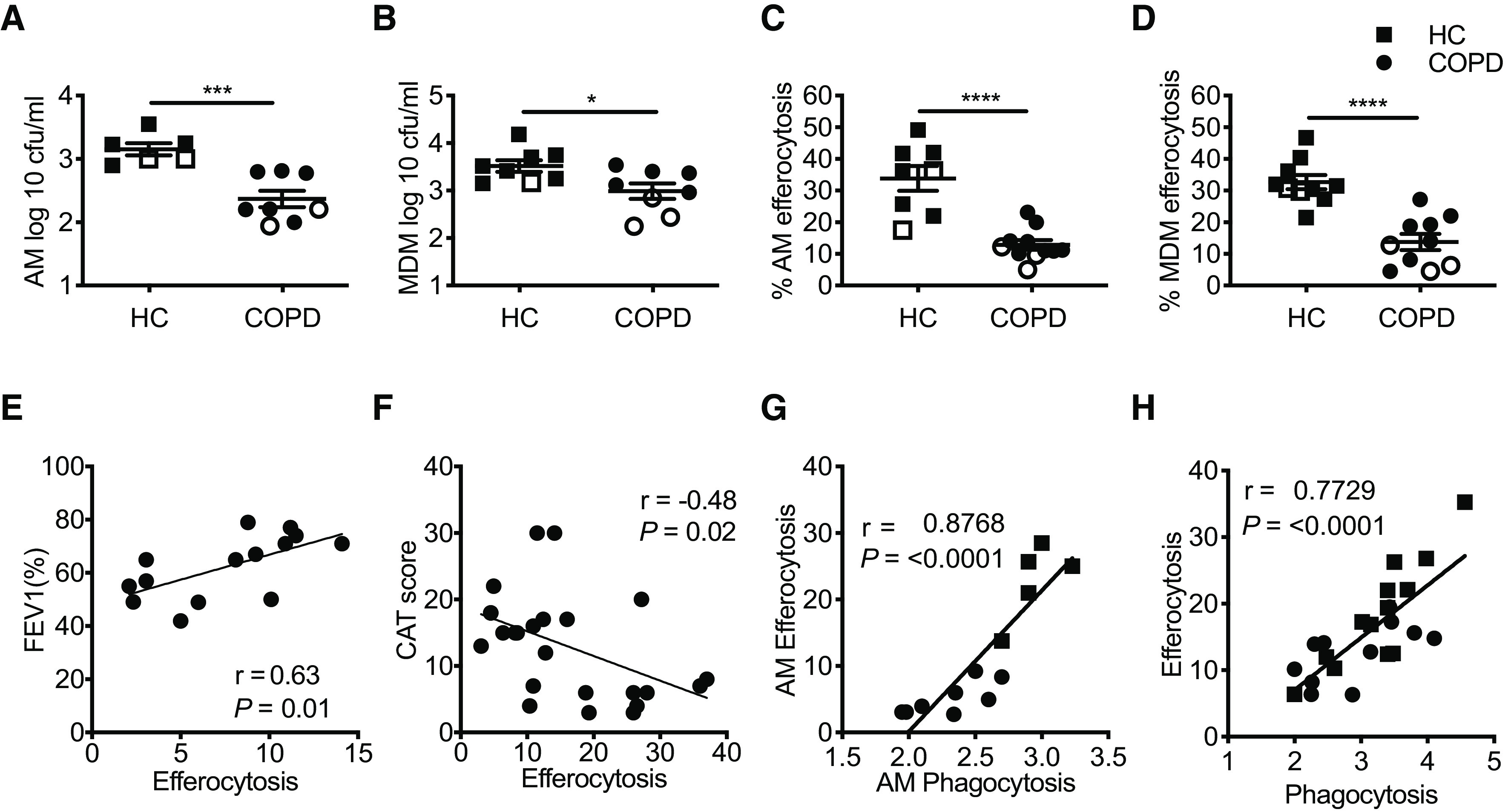
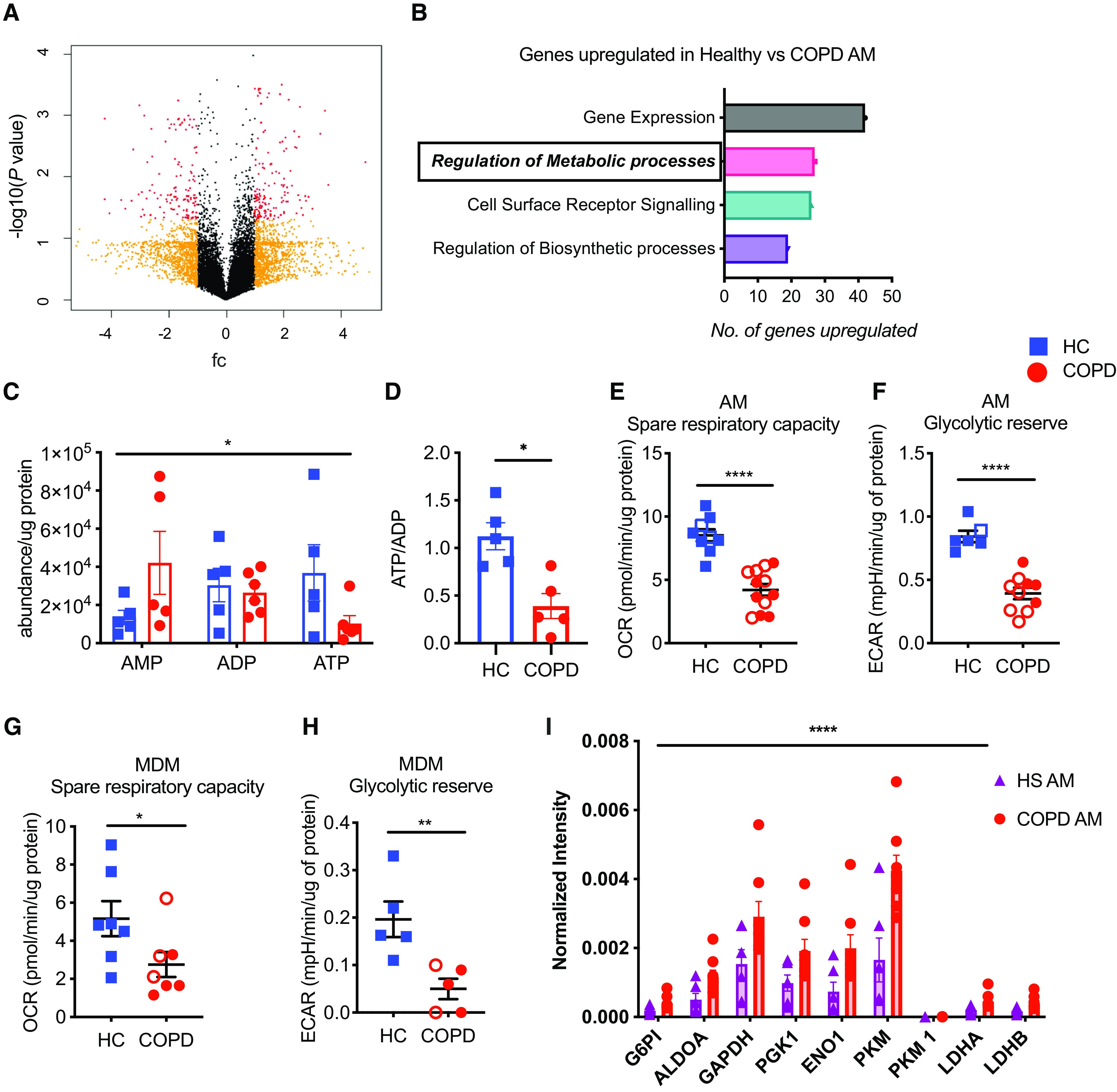
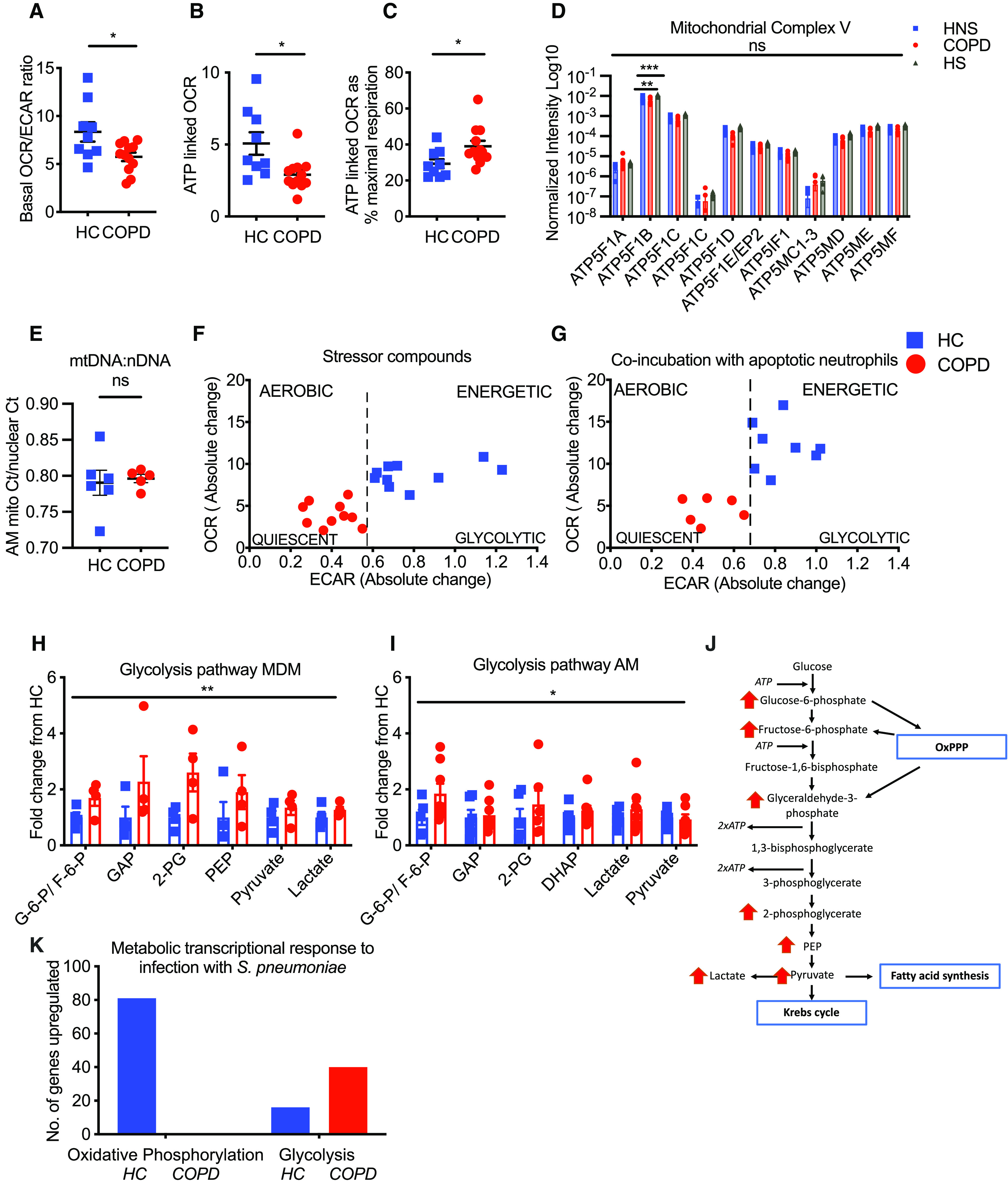
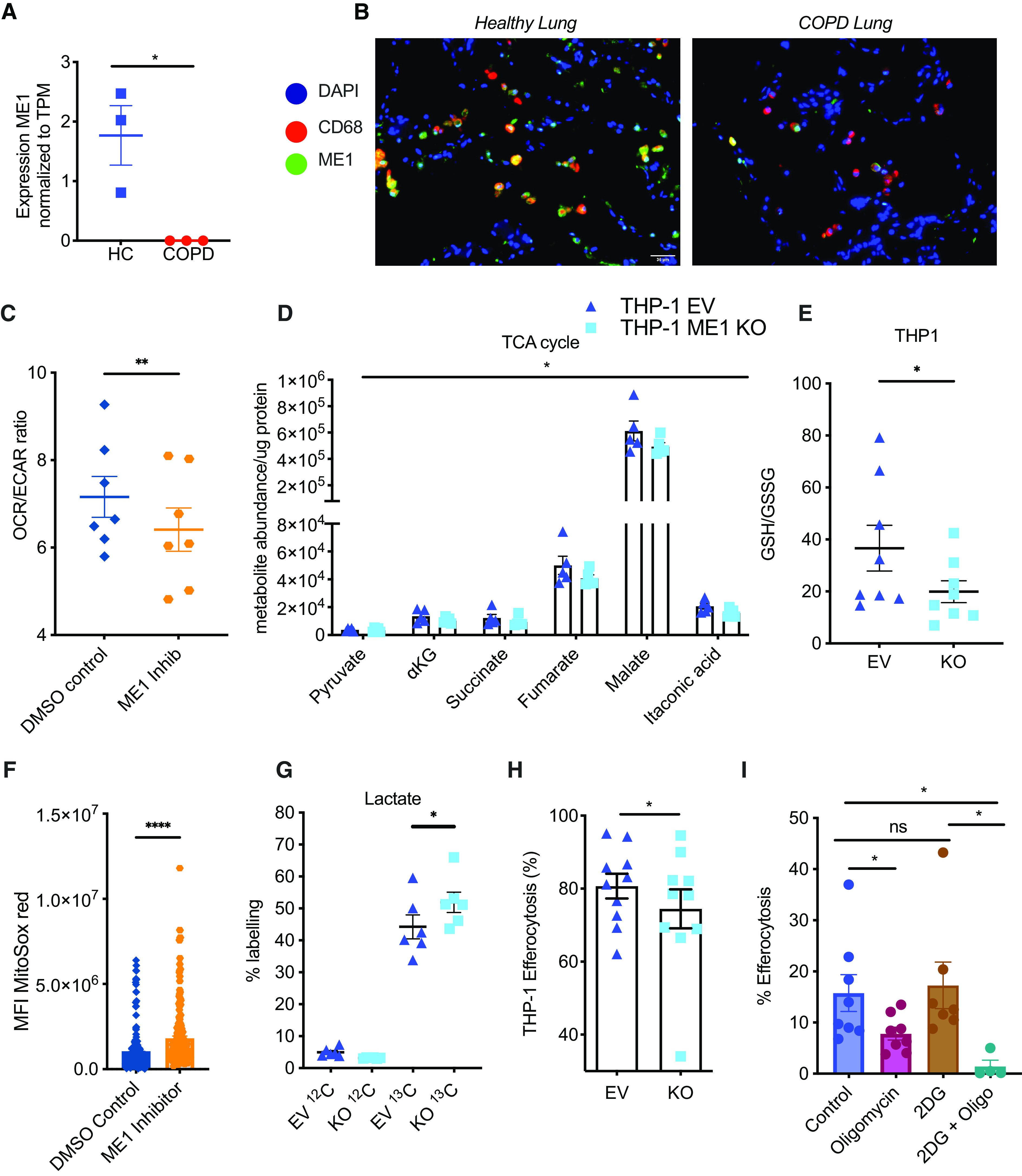
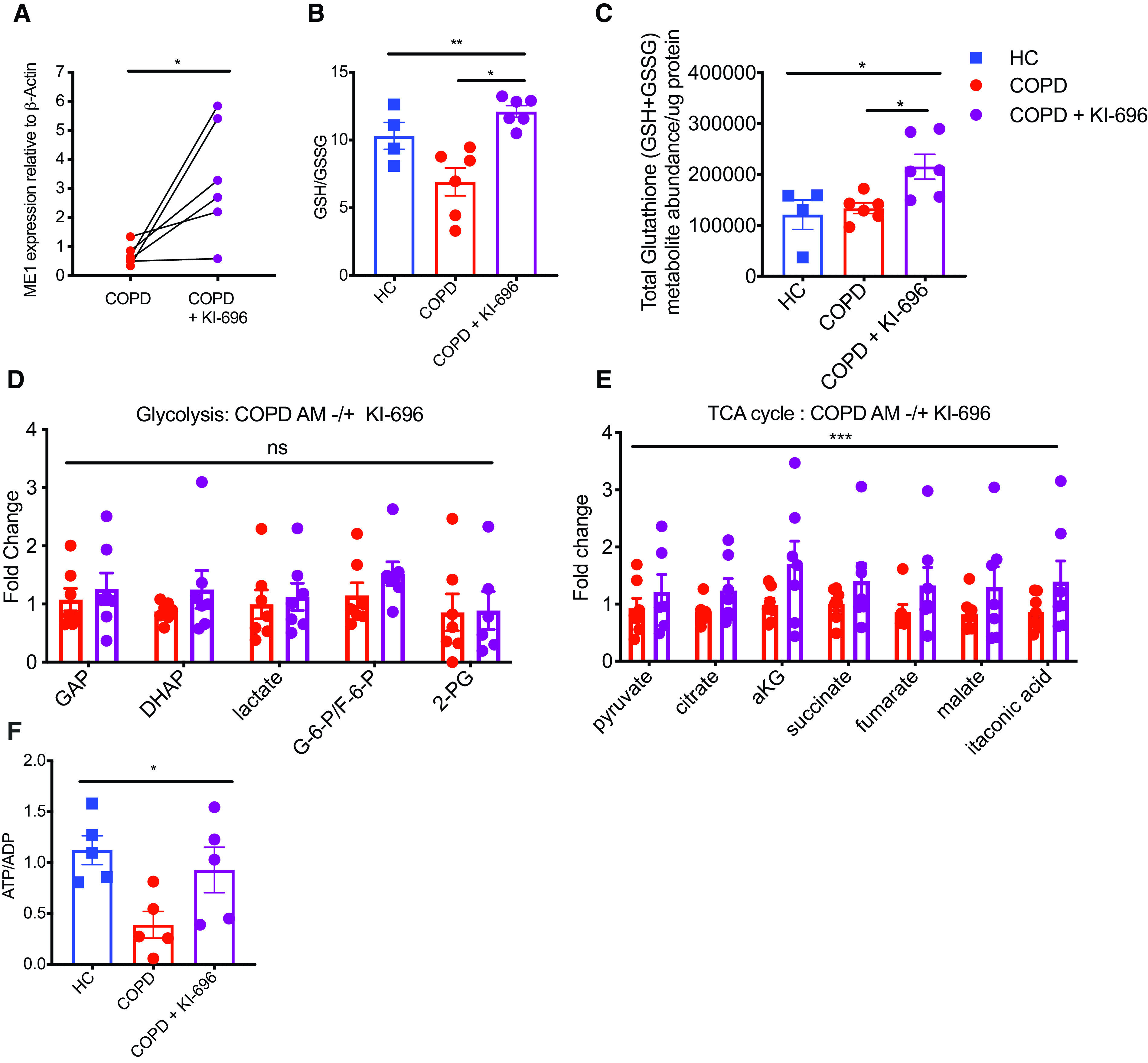
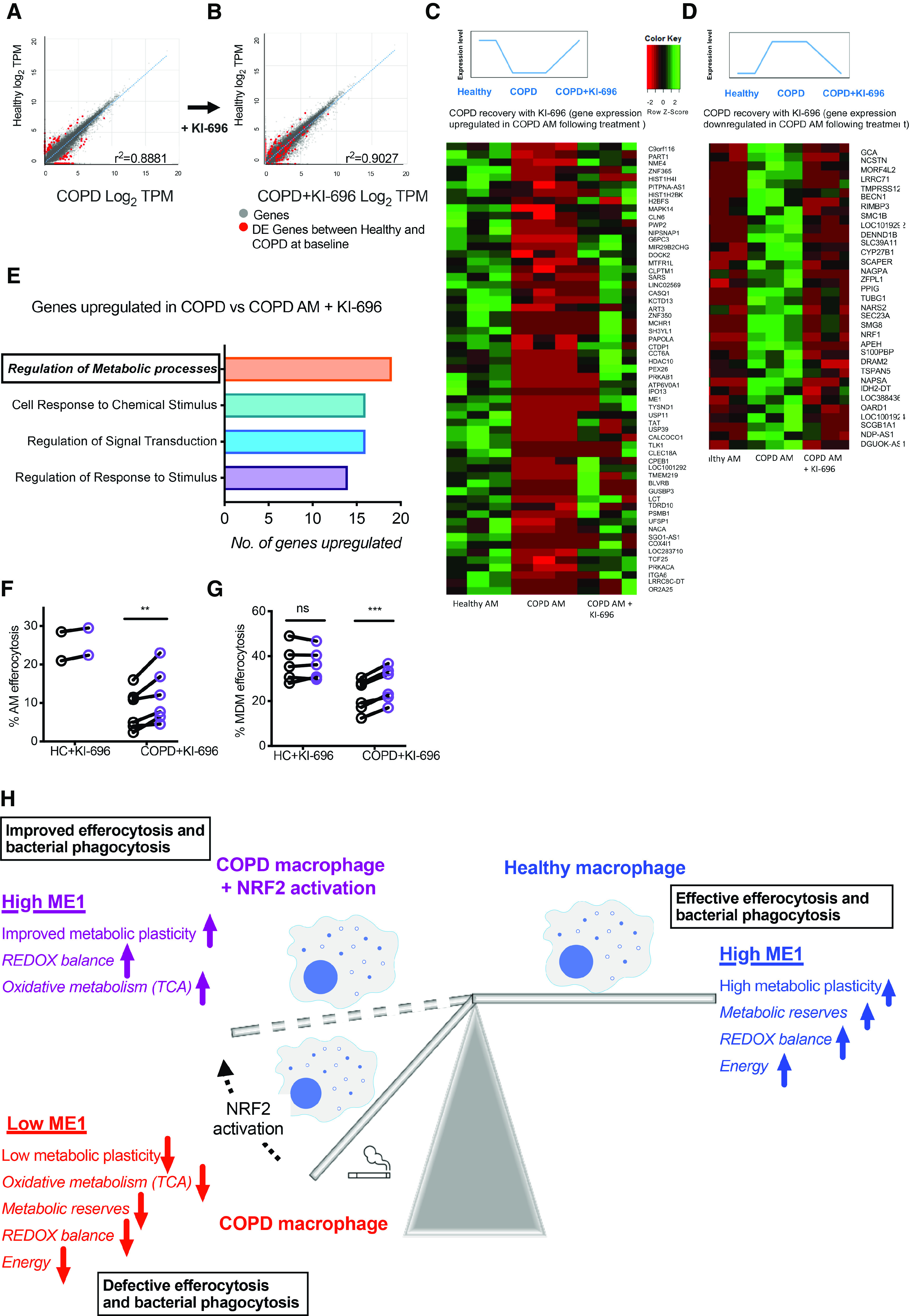
Rationale: Chronic obstructive pulmonary disease (COPD) is a disease characterized by persistent airway inflammation and disordered macrophage function. The extent to which alterations in macrophage bioenergetics contribute to impaired antioxidant responses and disease pathogenesis has yet to be fully delineated. Objectives: Through the study of COPD alveolar macrophages (AMs) and peripheral monocyte-derived macrophages (MDMs), we sought to establish if intrinsic defects in core metabolic processes drive macrophage dysfunction and redox imbalance. Methods: AMs and MDMs from donors with COPD and healthy donors underwent functional, metabolic, and transcriptional profiling. Measurements and Main Results: We observed that AMs and MDMs from donors with COPD display a critical depletion in glycolytic- and mitochondrial respiration-derived energy reserves and an overreliance on glycolysis as a source for ATP, resulting in reduced energy status. Defects in oxidative metabolism extend to an impaired redox balance associated with defective expression of the NADPH-generating enzyme, ME1 (malic enzyme 1), a known target of the antioxidant transcription factor NRF2 (nuclear factor erythroid 2-related factor 2). Consequently, selective activation of NRF2 resets the COPD transcriptome, resulting in increased generation of TCA cycle intermediaries, improved energetic status, favorable redox balance, and recovery of macrophage function. Conclusions: In COPD, an inherent loss of metabolic plasticity leads to metabolic exhaustion and reduced redox capacity, which can be rescued by activation of the NRF2 pathway. Targeting these defects, via NRF2 augmentation, may therefore present an attractive therapeutic strategy for the treatment of the aberrant airway inflammation described in COPD.
Keywords: COPD; macrophage; malic enzyme 1; metabolism; nuclear factor erythroid 2–related factor 2.
Figures
Comment in
-
"KEAP"ing Alveolar Macrophage Mitochondria Content in Chronic Obstructive Pulmonary Disease.Am J Respir Crit Care Med. 2023 Apr 15;207(8):962-964. doi: 10.1164/rccm.202302-0200ED. Am J Respir Crit Care Med. 2023. PMID: 36790378 Free PMC article. No abstract available.
References
-
- Willemse BW, ten Hacken NH, Rutgers B, Lesman-Leegte IG, Postma DS, Timens W. Effect of 1-year smoking cessation on airway inflammation in COPD and asymptomatic smokers. Eur Respir J . 2005;26:835–845. - PubMed
-
- Hogg JC, Chu F, Utokaparch S, Woods R, Elliott WM, Buzatu L, et al. The nature of small-airway obstruction in chronic obstructive pulmonary disease. N Engl J Med . 2004;350:2645–2653. - PubMed
-
- Oltmanns U, Sukkar MB, Xie S, John M, Chung KF. Induction of human airway smooth muscle apoptosis by neutrophils and neutrophil elastase. Am J Respir Cell Mol Biol . 2005;32:334–341. - PubMed
-
- Berenson CS, Garlipp MA, Grove LJ, Maloney J, Sethi S. Impaired phagocytosis of nontypeable Haemophilus influenzae by human alveolar macrophages in chronic obstructive pulmonary disease. J Infect Dis . 2006;194:1375–1384. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
