

Single-cell spatial landscapes of the lung tumour immune microenvironment
- PMID: 36725934
- PMCID: PMC9931585
- DOI: 10.1038/s41586-022-05672-3
Single-cell spatial landscapes of the lung tumour immune microenvironment
Abstract
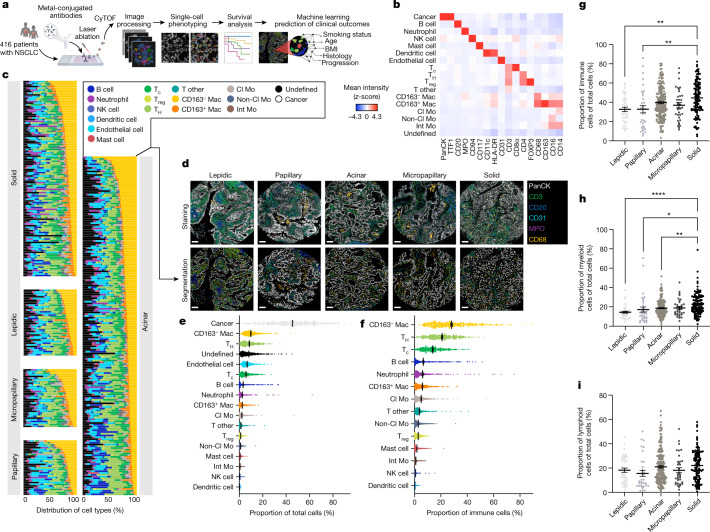
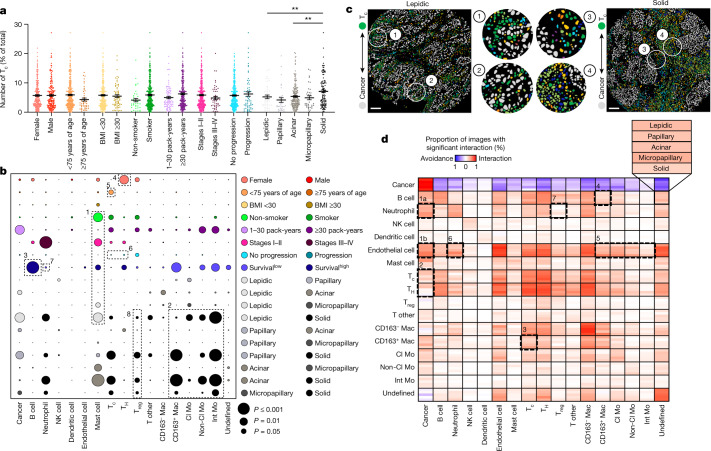
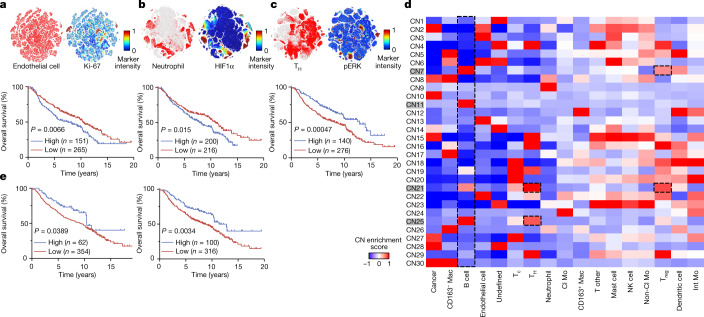
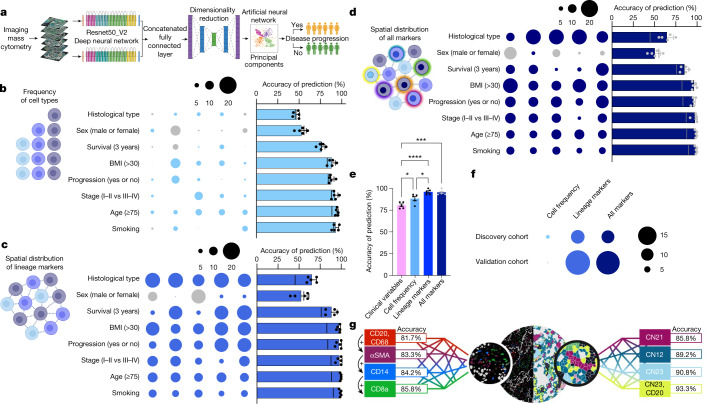
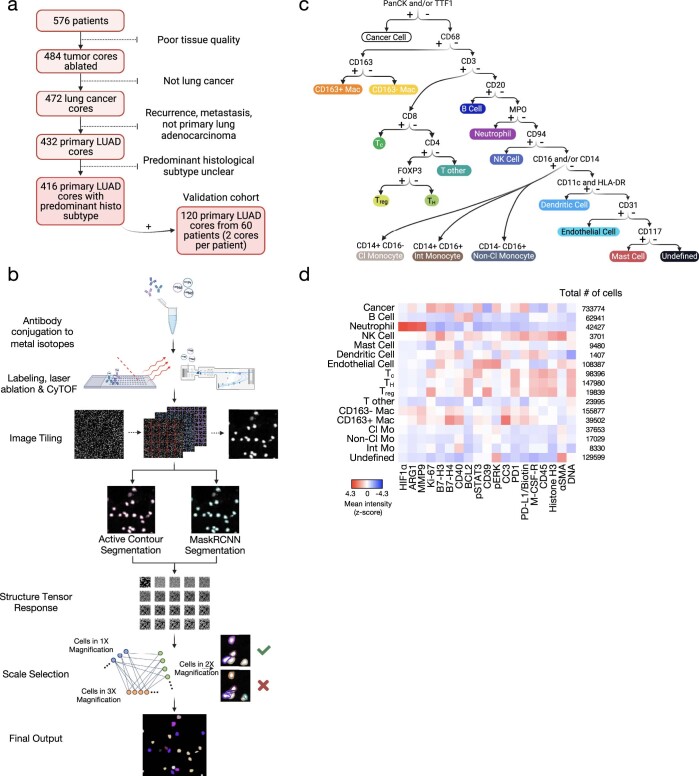
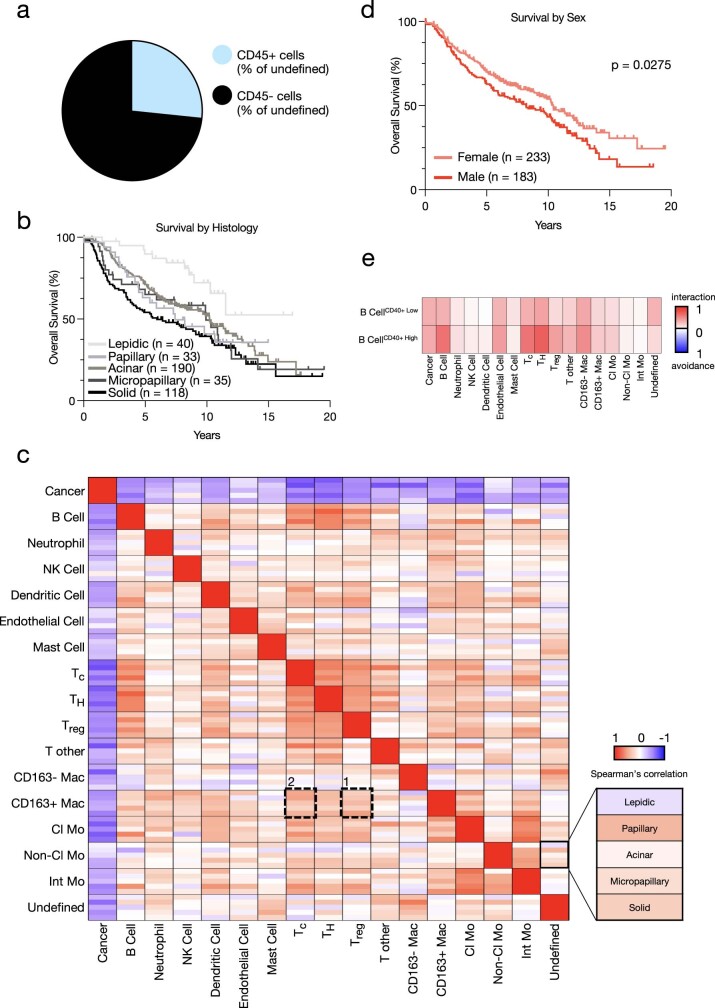
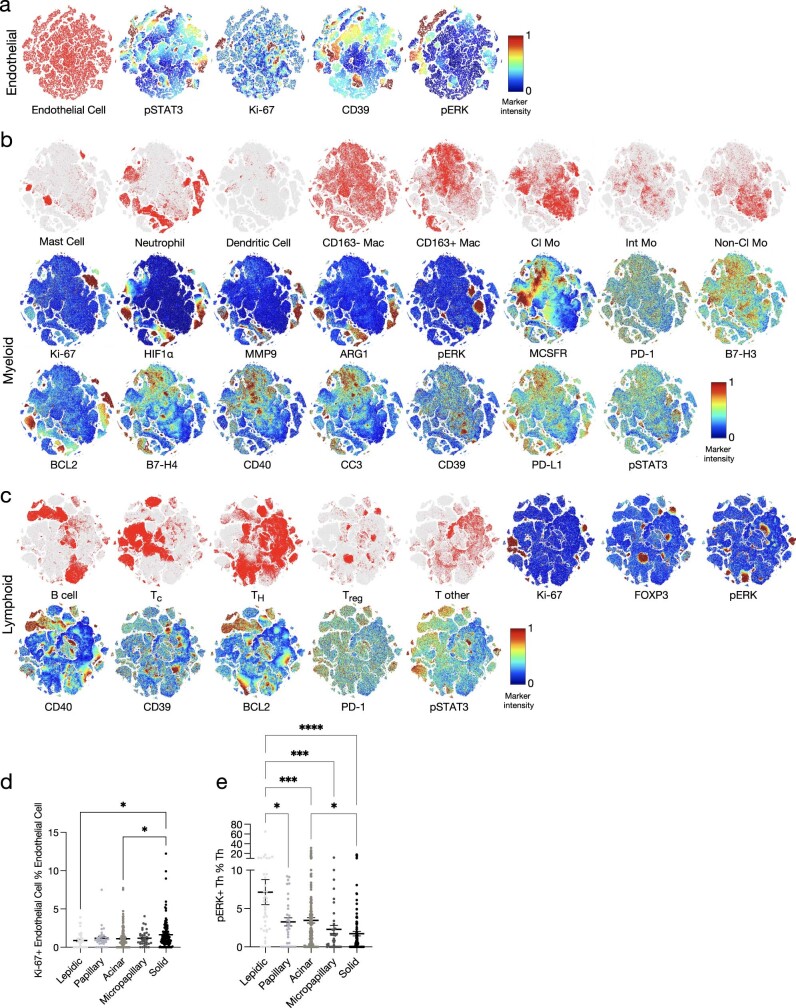
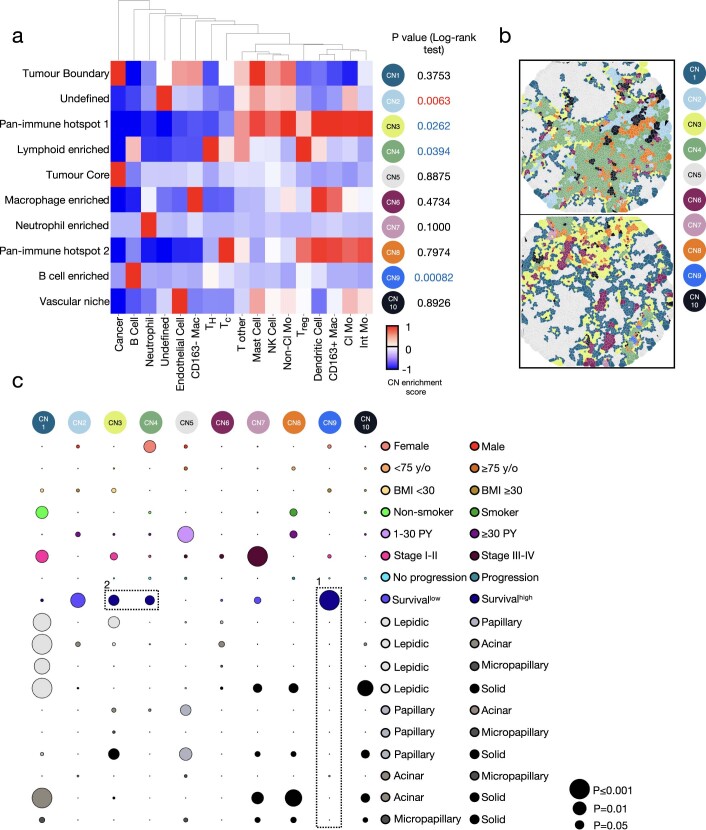
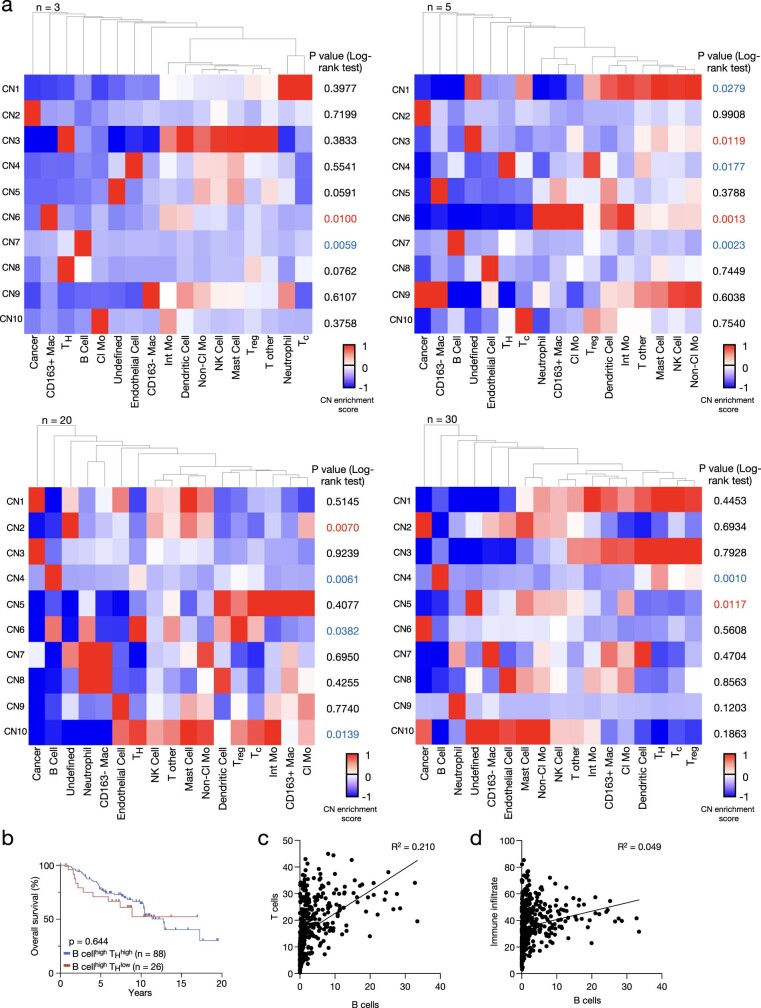
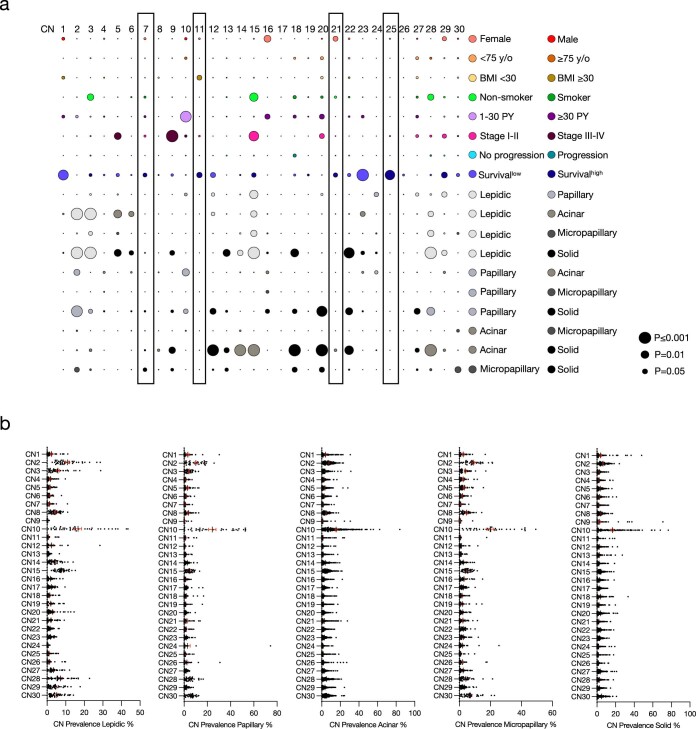
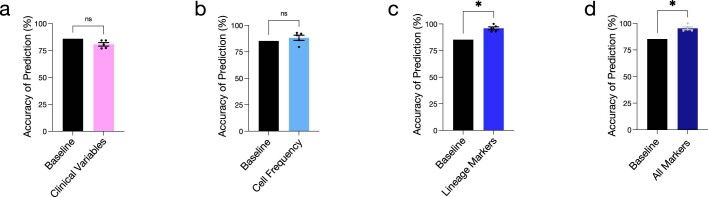
Single-cell technologies have revealed the complexity of the tumour immune microenvironment with unparalleled resolution1-9. Most clinical strategies rely on histopathological stratification of tumour subtypes, yet the spatial context of single-cell phenotypes within these stratified subgroups is poorly understood. Here we apply imaging mass cytometry to characterize the tumour and immunological landscape of samples from 416 patients with lung adenocarcinoma across five histological patterns. We resolve more than 1.6 million cells, enabling spatial analysis of immune lineages and activation states with distinct clinical correlates, including survival. Using deep learning, we can predict with high accuracy those patients who will progress after surgery using a single 1-mm2 tumour core, which could be informative for clinical management following surgical resection. Our dataset represents a valuable resource for the non-small cell lung cancer research community and exemplifies the utility of spatial resolution within single-cell analyses. This study also highlights how artificial intelligence can improve our understanding of microenvironmental features that underlie cancer progression and may influence future clinical practice.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interest.
Figures
Comment in
-
Spatial proteomics of tumor microenvironments reveal why location matters.Nat Immunol. 2023 Apr;24(4):565-566. doi: 10.1038/s41590-023-01471-8. Nat Immunol. 2023. PMID: 36959293 No abstract available.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
